Menon Prema, Narasimha Rao Katragadda Lakshmi, Samujh Ram, Yaddanapudi Sandhya
Department of Pediatric Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
Department of Anesthesia and Intensive Care, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
J Indian Assoc Pediatr Surg. 2022 Mar-Apr;27(2):173-179. doi: 10.4103/jiaps.JIAPS_356_20. Epub 2022 Mar 1.
The aim of the study is to compare the outcome in children born with long-gap esophageal atresia following reverse gastric tube esophagoplasty (RGTE) with or without the lower esophageal stump as a "fundoplication" wrap.
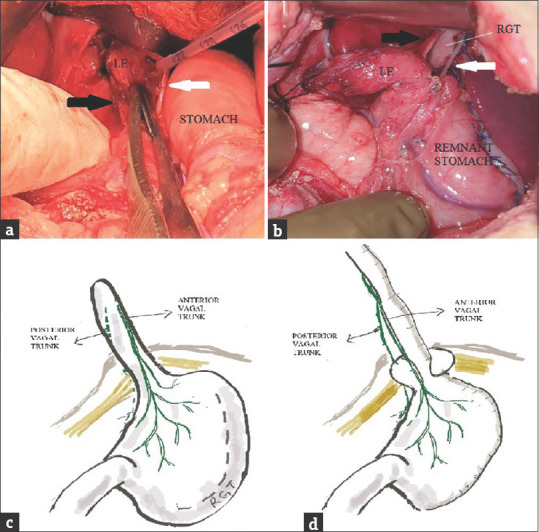
All children who underwent RGTE between 2008 and 2018 were retrospectively analyzed. Patients in whom the lower esophagus (LE) had been excised as is done routinely in RGTE (Group 1) were compared with those where the LE was wrapped partially or completely around the intraabdominal neo-esophagus (Group 2). Both vagal nerves were preserved to the extent possible. Complications and final outcome, including weight and height centiles were assessed. Follow-up upper gastrointestinal contrast study and reflux scans were studied.
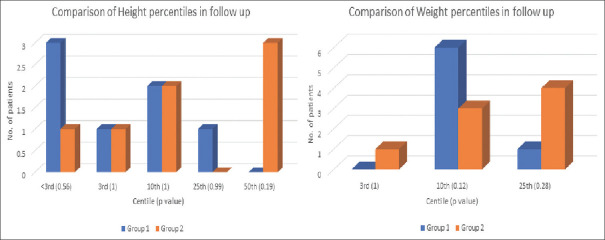
Nineteen patients (mean age: 15.78 ± 5.02 months [range 10-30 months] at RGTE) were studied; nine in Group 1 and ten in Group 2. Both groups had similar early postoperative complications as well as the requirement of dilatation for anastomotic stricture. Dysphagia for solids was noticed in two patients with complete lower esophageal wrap ( = 4), one requiring removal. More patients in Group 2 had absent reflux ( = 7) compared to Group 1 ( = 3) ( = 0.118). At a mean follow-up period of 45.75 ± 18.77 months (14-84 months), Group 2 children reached better height and weight percentiles compared to Group 1.
We have described a novel method of using the LE as a "fundoplication" wrap following RGTE. Vagi should be preserved. Those with complete esophageal wrap may develop dysphagia to solids and this is, therefore, not recommended. Lower esophageal wrap patients appeared to have a better outcome in terms of growth and less reflux.
本研究的目的是比较采用或不采用食管下段残端作为“胃底折叠术”包裹物的逆行胃管食管成形术(RGTE)治疗长间隙食管闭锁患儿的结局。
对2008年至2018年间接受RGTE治疗的所有患儿进行回顾性分析。将按照RGTE常规操作切除食管下段(LE)的患者(第1组)与食管下段部分或完全包裹在腹腔内新食管周围的患者(第2组)进行比较。尽可能保留双侧迷走神经。评估并发症和最终结局,包括体重和身高百分位数。研究随访期间的上消化道造影研究和反流扫描。
研究了19例患者(RGTE时平均年龄:15.78±5.02个月[范围10 - 30个月]);第1组9例,第2组10例。两组术后早期并发症相似,吻合口狭窄扩张需求也相似。两名食管下段完全包裹的患者出现固体食物吞咽困难(= 4),其中一名需要移除包裹物。与第1组(= 3)相比,第2组无反流的患者更多(= 7)(= 0.118)。平均随访期为45.75±18.77个月(14 - 84个月),第2组患儿的身高和体重百分位数高于第1组。
我们描述了一种在RGTE后使用食管下段作为“胃底折叠术”包裹物的新方法。应保留迷走神经。食管完全包裹的患者可能会出现固体食物吞咽困难,因此不推荐这样做。食管下段包裹的患者在生长和反流较少方面似乎有更好的结局。