Department of Pediatrics, ISN-SRC, All India Institute of Medical Sciences (AIIMS), Room no 1023, Academic Block, Saket Nagar, Bhopal, MP, 462024, India.
Advanced Pediatrics Centre, Division of Clinical Immunology and Rheumatology, Post Graduate Institute of Medical Sciences (PGI), Chandigarh, India.
Pediatr Nephrol. 2023 Feb;38(2):357-370. doi: 10.1007/s00467-022-05701-3. Epub 2022 Aug 9.
Multisystem inflammatory syndrome (MIS-C) is a rare paediatric hyper-inflammatory disorder that occurs following SARS-CoV-2 infection. Acute kidney injury (AKI) occurs in approximately one-quarter to one-third of the patients with MIS-C and is associated with poor prognosis in critically ill children. This systematic review is aimed to evaluate the incidence of AKI, mortality, and the need for kidney replacement therapy (KRT) in patients with MIS-C.
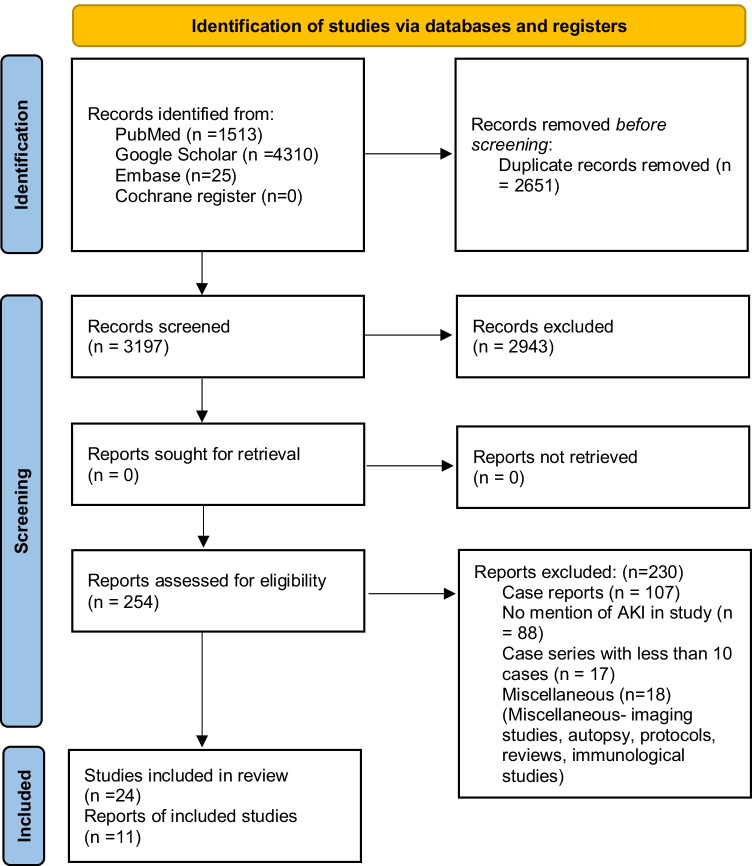
We searched databases from Medline, EMBASE, Cochrane Register, and Google Scholar from December 2019 to December 2021 with our search strategy. Studies meeting the following criteria were included in this systematic review: (1) articles on AKI in MIS-C; (2) studies providing AKI in MIS-C and COVID-19 infection separately; (3) studies reporting outcomes such as mortality, KRT, serum creatinine; length of hospital/ICU stay.
The quality of the included studies was independently assessed by using the National Heart Lung and Blood Institute (NHLBI) quality assessment tool for cohort studies and case series.
Outcomes and their 95% confidence intervals (CI) were reported if a meta-analysis of these outcomes was conducted. Heterogeneity was reported using I statistics, and heterogeneity ≥ 50% was considered high. We used Baujat's plot for the contribution of each study toward overall heterogeneity. In sensitivity analysis, the summary estimates were assessed by repeating meta-analysis after omitting one study at a time. Forest plots were used for reporting outcomes in each study and with their 95% CI. All statistical tests were performed using R software version 4.0.3.
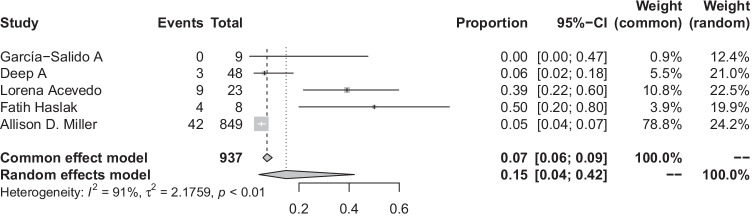
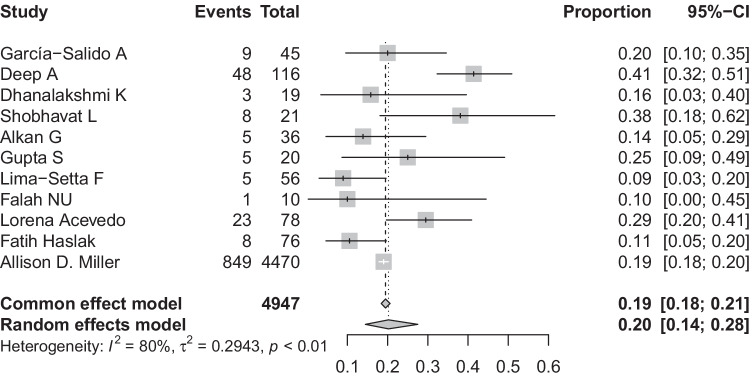
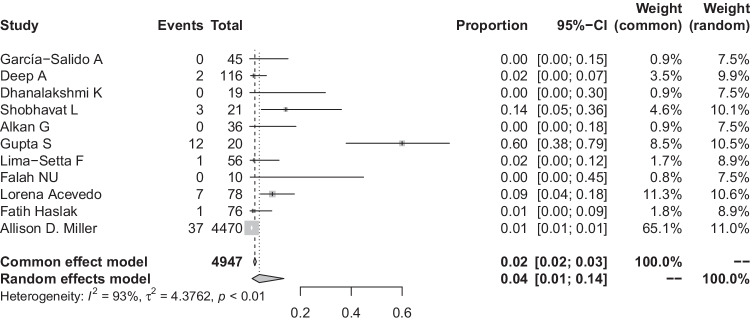
A total of 24 studies were included in this systematic review and of these, 11 were included in the meta-analysis. The pooled proportion of patients with MIS-C developing AKI was 20% (95% CI: 14-28%, I = 80%). Pooled proportion of death in children with MIS-C was 4% (95% CI: 1-14%; I = 93%). The odds of death in patients with AKI were 4.68 times higher than in patients without AKI (95% CI: 1.06-20.7%; I = 17%). The overall pooled proportion of MIS-C-induced AKI patients requiring KRT was 15% (95% CI: 4-42%; I = 91%).
Approximately one-fifth of children with MIS-C develop AKI which is associated with higher odds of death. PROSPERO registration: CRD42022306170 A higher resolution version of the Graphical abstract is available as Supplementary information.
儿童多系统炎症综合征(MIS-C)是一种罕见的儿科超炎症性疾病,发生在 SARS-CoV-2 感染后。大约四分之一至三分之一的 MIS-C 患者会出现急性肾损伤(AKI),并且在危重病儿童中与预后不良相关。本系统评价旨在评估 MIS-C 患者 AKI 的发生率、死亡率和肾脏替代治疗(KRT)的需求。
我们从 Medline、EMBASE、Cochrane 注册中心和 Google Scholar 数据库中检索了 2019 年 12 月至 2021 年 12 月的文献,检索策略如下。本系统评价纳入了符合以下标准的研究:(1)关于 MIS-C 中 AKI 的文章;(2)分别提供 MIS-C 和 COVID-19 感染中 AKI 的研究;(3)报告死亡率、KRT、血清肌酐等结局的研究;住院/ICU 时间。
使用美国国立心肺血液研究所(NHLBI)队列研究和病例系列质量评估工具独立评估纳入研究的质量。
如果对这些结局进行了荟萃分析,则报告结局和它们的 95%置信区间(CI)。使用 I 统计量报告异质性,如果 I 统计量≥50%,则认为存在高度异质性。我们使用 Baujat 的图来评估每个研究对总体异质性的贡献。在敏感性分析中,通过每次删除一项研究来重新进行荟萃分析,评估汇总估计值。森林图用于报告每个研究的结局及其 95%CI。所有统计检验均使用 R 软件版本 4.0.3 进行。
本系统评价共纳入 24 项研究,其中 11 项纳入荟萃分析。MIS-C 患者发生 AKI 的患者比例为 20%(95%CI:14-28%,I=80%)。MIS-C 患儿死亡的合并比例为 4%(95%CI:1-14%;I=93%)。AKI 患者死亡的几率是无 AKI 患者的 4.68 倍(95%CI:1.06-20.7%;I=17%)。MIS-C 引起的 AKI 患者需要 KRT 的总体合并比例为 15%(95%CI:4-42%;I=91%)。
大约五分之一的 MIS-C 患儿会发生 AKI,这与更高的死亡几率相关。PROSPERO 注册:CRD42022306170 更清晰的图表版本可在补充信息中查看。