Rhedin Samuel, Lundholm Cecilia, Horne AnnaCarin, Smew Awad I, Osvald Emma Caffrey, Haddadi Araz, Alfvén Tobias, Kahn Robin, Król Petra, Brew Bronwyn Haasdyk, Almqvist Catarina
Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
Sachs' Children and Youth Hospital, Stockholm, Sweden.
Lancet Reg Health Eur. 2022 Aug;19:100443. doi: 10.1016/j.lanepe.2022.100443. Epub 2022 Jun 22.
Although severe acute COVID-19 is rare in children, SARS-CoV-2 infection can trigger the novel post-infectious condition multisystem inflammatory syndrome in children (MIS-C). Increased knowledge on risk factors for MIS-C could improve our understanding of the pathogenesis of the condition and better guide targeted public health interventions. The aim of the study was to assess risk factors for MIS-C with the aim to identify vulnerable children.
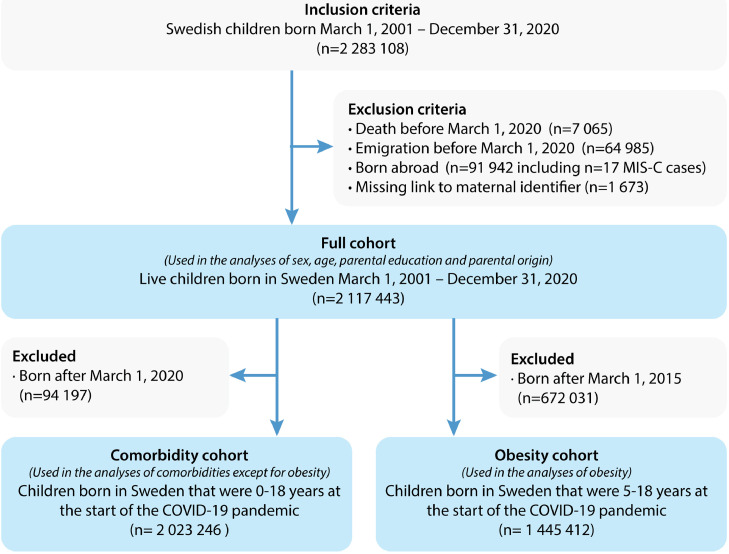
A register-based cohort study including all children and adolescents <19 years born in Sweden between March 1, 2001- December 31, 2020 was performed. Data on sociodemographic risk factors and comorbidities (sex, age, parental region of birth, parental education, asthma, autoimmune disease, chromosomal anomalies, chronic heart disease, chronic lung disease, obesity, life-limiting condition) were retrieved from national health and population registers. The outcome was MIS-C diagnosis according to the Swedish Pediatric Rheumatology Quality Register during March 1, 2020 - December 8, 2021.Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using Cox regression analysis. Incidence rates per 100 000 person-years were calculated assuming a Poisson distribution.
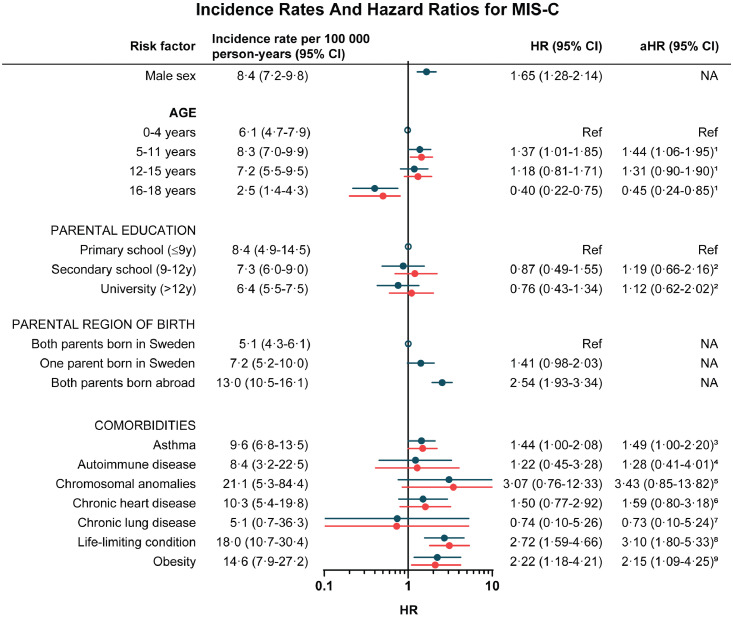
Among 2 117 443 children included in the study, 253 children developed MIS-C, corresponding to an incidence rate of 6·8 (95% CI: 6·0-7·6) per 100 000 person-years. Male sex (HR 1·65, 95% CI: 1·28-2·14), age 5-11 years (adjusted HR 1·44, 95% CI: 1·06-1·95 using children 0-4 years as reference), foreign-born parents (HR 2·53, 95% CI: 1·93-3·34), asthma (aHR 1·49, 95% CI: 1·00-2·20), obesity (aHR 2·15, 95% CI: 1·09-4·25) and life-limiting conditions (aHR 3·10, 95% CI: 1·80-5·33) were associated with MIS-C. Children 16-18 years had a reduced risk for MIS-C (aHR 0·45, 95% CI: 0·24-0·85).
We report increased risks for MIS-C in children with male sex, age 5-11 years, foreign-born parents, asthma, obesity, and life-limiting condition. Knowing these risk populations might facilitate identification of children with MIS-C and potentially guide targeted public health interventions. Nevertheless, the absolute risks for MIS-C were very low.
Financial support was provided from the Swedish Research Council (grant no 2018-02640), the Swedish Heart-Lung Foundation (grant no 20210416), the Asthma and Allergy Association, Ake Wiberg foundation, the Samariten Foundation, the Society of Child Care, and Region Stockholm.
尽管儿童严重急性新冠病毒病(COVID-19)较为罕见,但严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染可引发儿童新型感染后病症——儿童多系统炎症综合征(MIS-C)。增加对MIS-C危险因素的了解,有助于我们更好地理解该病症的发病机制,并更有效地指导针对性的公共卫生干预措施。本研究旨在评估MIS-C的危险因素,以识别易患儿童。
开展一项基于登记的队列研究,纳入2001年3月1日至2020年12月31日在瑞典出生的所有19岁以下儿童和青少年。从国家卫生和人口登记处获取社会人口学危险因素和合并症(性别、年龄、父母出生地、父母教育程度、哮喘、自身免疫性疾病、染色体异常、慢性心脏病、慢性肺病、肥胖、危及生命的疾病)的数据。研究结局为2020年3月1日至2021年12月8日期间瑞典儿科风湿病质量登记处记录的MIS-C诊断。使用Cox回归分析计算风险比(HR)和95%置信区间(CI)。假设为泊松分布,计算每10万人年的发病率。
在纳入研究的2117443名儿童中,253名儿童发生了MIS-C,发病率为每10万人年6.8例(95%CI:6.0 - 7.6)。男性(HR 1.65,95%CI:1.28 - 2.14)、5 - 11岁儿童(以0 - 4岁儿童为参照,调整后HR 1.44,95%CI:1.06 - 1.95)、父母为外国出生(HR 2.53,95%CI:1.93 - 3.34)、哮喘(调整后HR 1.49,95%CI:1.00 - 2.20)、肥胖(调整后HR 2.15,95%CI:1.09 - 4.25)和危及生命的疾病(调整后HR 3.10,95%CI:1.80 - 5.33)与MIS-C相关。16 - 18岁儿童患MIS-C的风险降低(调整后HR 0.45,95%CI:0.24 - 0.85)。
我们报告了男性、5 - 11岁儿童、父母为外国出生、哮喘、肥胖和患有危及生命疾病的儿童发生MIS-C的风险增加。了解这些风险人群可能有助于识别MIS-C患儿,并可能指导针对性的公共卫生干预措施。然而,MIS-C的绝对风险非常低。
本研究得到瑞典研究理事会(资助编号2018 - 02640)、瑞典心肺基金会(资助编号20210416)、哮喘与过敏协会、阿克·维伯格基金会、撒玛利亚人基金会、儿童护理协会以及斯德哥尔摩地区的资助。