Section of Critical Care Medicine, Department of Pediatrics, University of Colorado School of Medicine, University of Colorado, Aurora.
Section of Informatics and Data Science, Department of Pediatrics, University of Colorado School of Medicine, University of Colorado, Aurora.
JAMA Netw Open. 2022 Feb 1;5(2):e2143151. doi: 10.1001/jamanetworkopen.2021.43151.
Understanding of SARS-CoV-2 infection in US children has been limited by the lack of large, multicenter studies with granular data.
To examine the characteristics, changes over time, outcomes, and severity risk factors of children with SARS-CoV-2 within the National COVID Cohort Collaborative (N3C).
DESIGN, SETTING, AND PARTICIPANTS: A prospective cohort study of encounters with end dates before September 24, 2021, was conducted at 56 N3C facilities throughout the US. Participants included children younger than 19 years at initial SARS-CoV-2 testing.
Case incidence and severity over time, demographic and comorbidity severity risk factors, vital sign and laboratory trajectories, clinical outcomes, and acute COVID-19 vs multisystem inflammatory syndrome in children (MIS-C), and Delta vs pre-Delta variant differences for children with SARS-CoV-2.
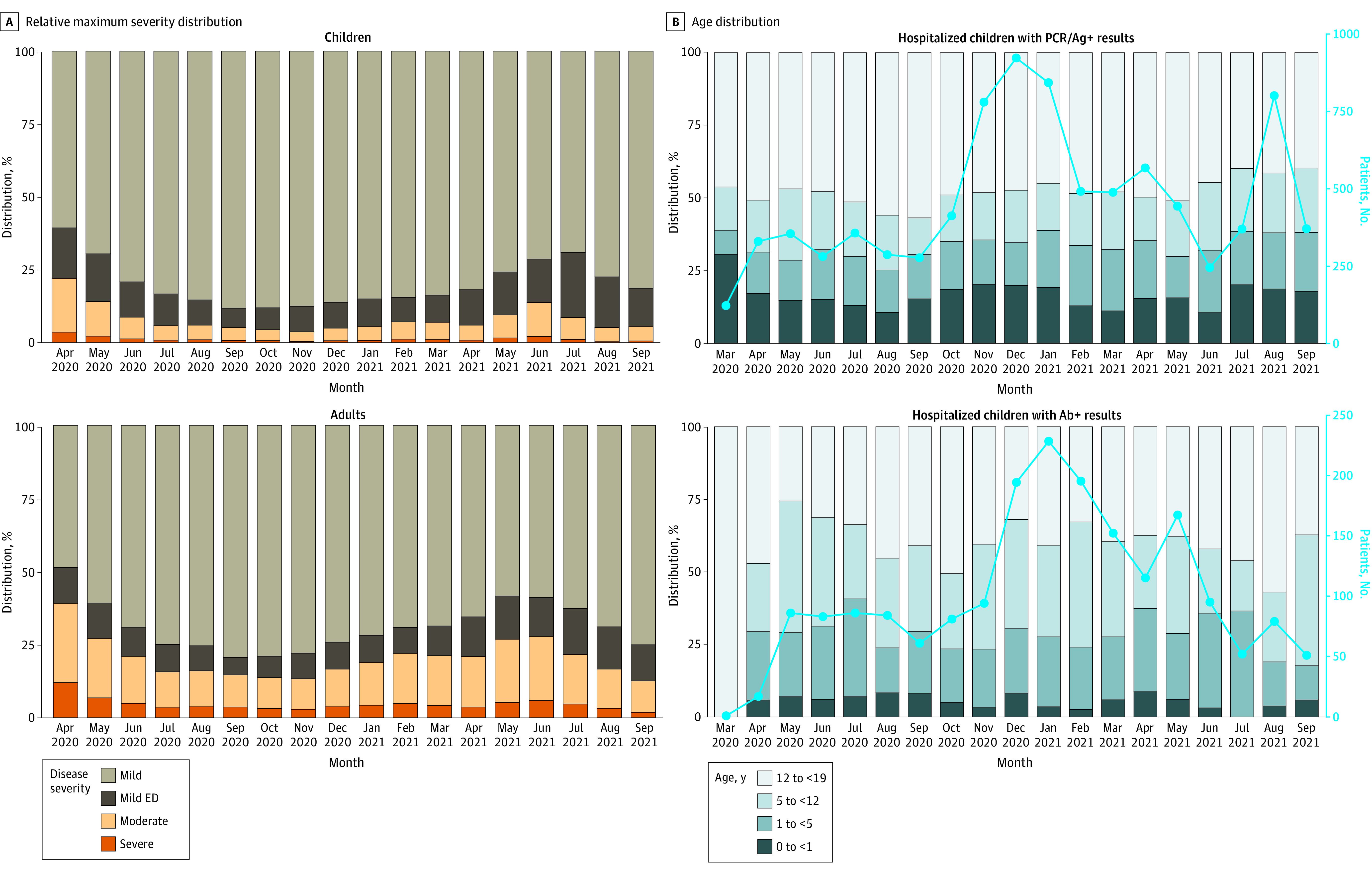
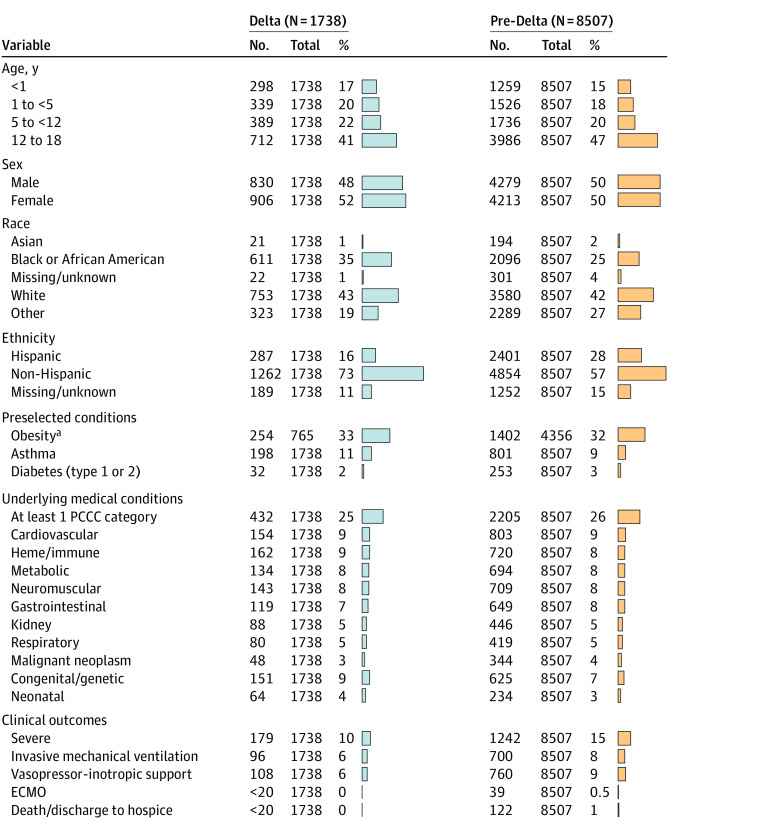
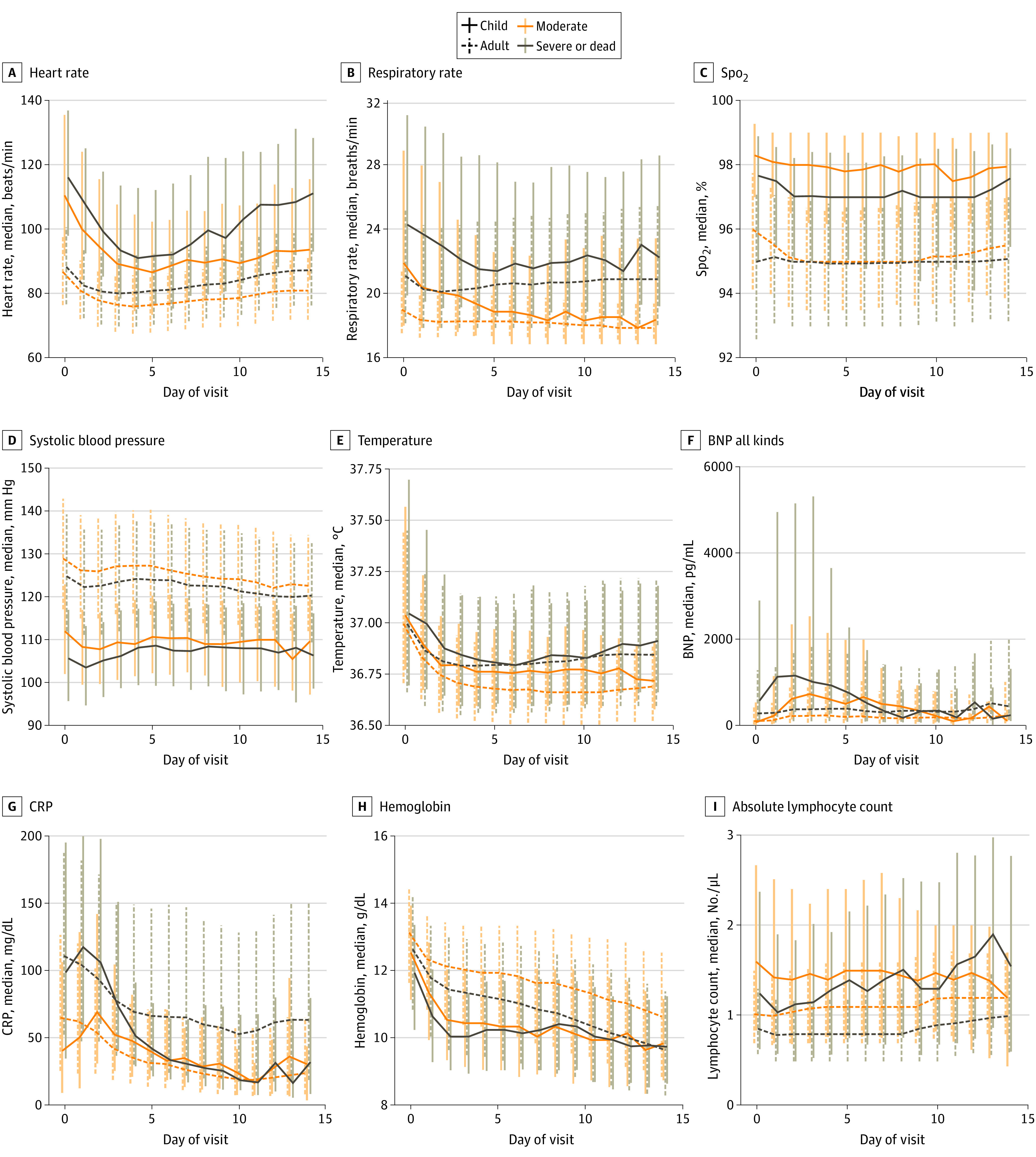
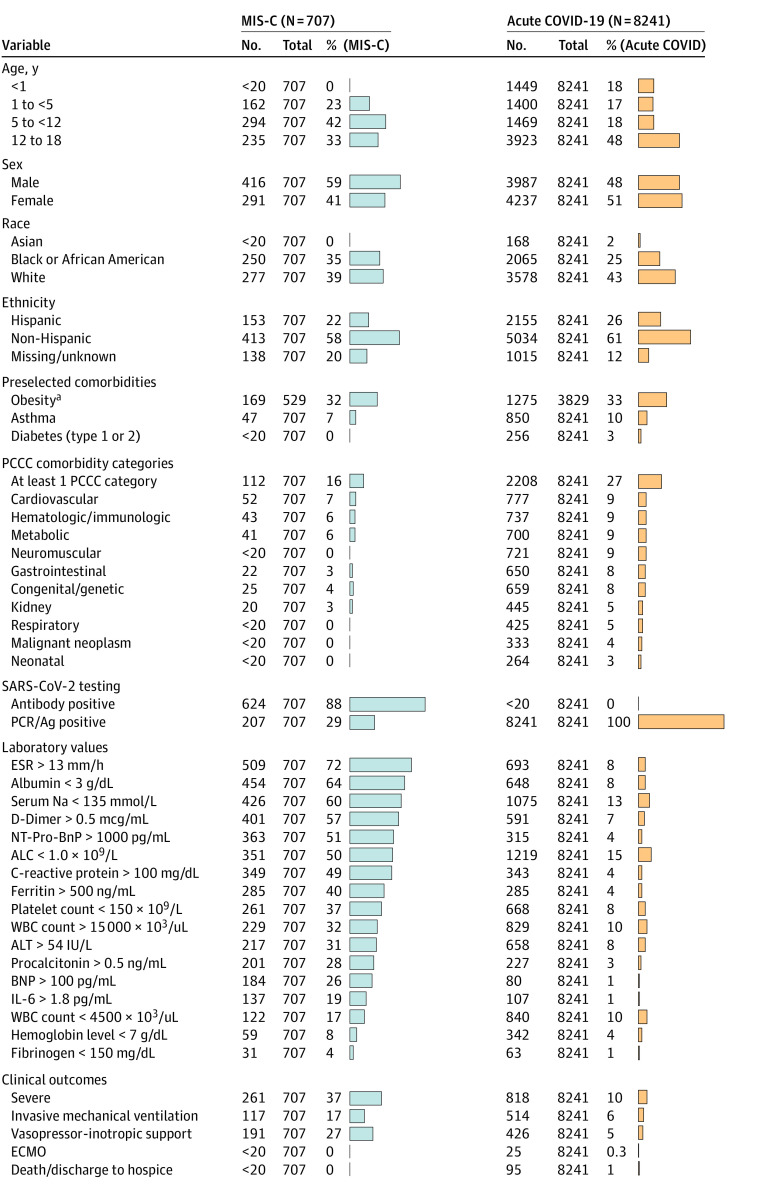
A total of 1 068 410 children were tested for SARS-CoV-2 and 167 262 test results (15.6%) were positive (82 882 [49.6%] girls; median age, 11.9 [IQR, 6.0-16.1] years). Among the 10 245 children (6.1%) who were hospitalized, 1423 (13.9%) met the criteria for severe disease: mechanical ventilation (796 [7.8%]), vasopressor-inotropic support (868 [8.5%]), extracorporeal membrane oxygenation (42 [0.4%]), or death (131 [1.3%]). Male sex (odds ratio [OR], 1.37; 95% CI, 1.21-1.56), Black/African American race (OR, 1.25; 95% CI, 1.06-1.47), obesity (OR, 1.19; 95% CI, 1.01-1.41), and several pediatric complex chronic condition (PCCC) subcategories were associated with higher severity disease. Vital signs and many laboratory test values from the day of admission were predictive of peak disease severity. Variables associated with increased odds for MIS-C vs acute COVID-19 included male sex (OR, 1.59; 95% CI, 1.33-1.90), Black/African American race (OR, 1.44; 95% CI, 1.17-1.77), younger than 12 years (OR, 1.81; 95% CI, 1.51-2.18), obesity (OR, 1.76; 95% CI, 1.40-2.22), and not having a pediatric complex chronic condition (OR, 0.72; 95% CI, 0.65-0.80). The children with MIS-C had a more inflammatory laboratory profile and severe clinical phenotype, with higher rates of invasive ventilation (117 of 707 [16.5%] vs 514 of 8241 [6.2%]; P < .001) and need for vasoactive-inotropic support (191 of 707 [27.0%] vs 426 of 8241 [5.2%]; P < .001) compared with those who had acute COVID-19. Comparing children during the Delta vs pre-Delta eras, there was no significant change in hospitalization rate (1738 [6.0%] vs 8507 [6.2%]; P = .18) and lower odds for severe disease (179 [10.3%] vs 1242 [14.6%]) (decreased by a factor of 0.67; 95% CI, 0.57-0.79; P < .001).
In this cohort study of US children with SARS-CoV-2, there were observed differences in demographic characteristics, preexisting comorbidities, and initial vital sign and laboratory values between severity subgroups. Taken together, these results suggest that early identification of children likely to progress to severe disease could be achieved using readily available data elements from the day of admission. Further work is needed to translate this knowledge into improved outcomes.
由于缺乏具有详细数据的大型多中心研究,美国儿童对 SARS-CoV-2 感染的了解受到限制。
通过国家 COVID 队列协作(N3C)研究,检查美国 56 个 N3C 设施中 SARS-CoV-2 儿童的特征、随时间的变化、结局和严重程度的危险因素。
设计、地点和参与者:前瞻性队列研究,参与者为首次 SARS-CoV-2 检测时年龄小于 19 岁的儿童。
严重程度随时间的变化、人口统计学和合并症严重程度危险因素、生命体征和实验室轨迹、临床结局以及急性 COVID-19 与儿童多系统炎症综合征(MIS-C)之间的区别,以及 SARS-CoV-2 儿童 Delta 与前 Delta 变异之间的区别。
共有 1068410 名儿童接受了 SARS-CoV-2 检测,167262 项检测结果(15.6%)呈阳性(82882[49.6%]名女孩;中位年龄,11.9[IQR,6.0-16.1]岁)。在 10245 名住院患儿中,1423 名(13.9%)符合严重疾病标准:机械通气(796[7.8%])、血管活性药物支持(868[8.5%])、体外膜氧合(42[0.4%])或死亡(131[1.3%])。男性(优势比[OR],1.37;95%CI,1.21-1.56)、黑种人/非裔美国人(OR,1.25;95%CI,1.06-1.47)、肥胖(OR,1.19;95%CI,1.01-1.41)和多种儿科复杂慢性疾病(PCCC)亚类与更高的严重疾病相关。入院当天的生命体征和许多实验室检查值均可预测疾病高峰的严重程度。与急性 COVID-19 相比,与 MIS-C 相关的变量包括男性(OR,1.59;95%CI,1.33-1.90)、黑种人/非裔美国人(OR,1.44;95%CI,1.17-1.77)、年龄小于 12 岁(OR,1.81;95%CI,1.51-2.18)、肥胖(OR,1.76;95%CI,1.40-2.22)和没有儿科复杂慢性疾病(OR,0.72;95%CI,0.65-0.80)。MIS-C 患儿具有更具炎症性的实验室特征和严重的临床表型,需要进行侵入性通气的比例更高(707 例中有 117 例[16.5%],8241 例中有 514 例[6.2%];P<.001)和需要血管活性药物支持的比例更高(707 例中有 191 例[27.0%],8241 例中有 426 例[5.2%];P<.001),而急性 COVID-19 患儿中只有 117 例(16.5%)和 426 例(5.2%)。与 Delta 时代相比,Delta 时代的住院率没有明显变化(1738[6.0%] vs 8507[6.2%];P=.18),严重疾病的几率也降低(179[10.3%] vs 1242[14.6%])(降低了 0.67 倍;95%CI,0.57-0.79;P<.001)。
在这项针对美国儿童 SARS-CoV-2 的队列研究中,严重程度亚组之间的人口统计学特征、合并症严重程度和初始生命体征和实验室值存在差异。综上所述,这些结果表明,使用入院当天的可用数据元素,可以早期识别可能发展为严重疾病的儿童。需要进一步的工作来将这些知识转化为改善的结局。