Department of Anesthesiology and Critical Care, The University of Pennsylvania, JMB 127, 3620 Hamilton Walk, Philadelphia, PA, 19146, USA.
Leonard Davis Institute for Health Economics, The University of Pennsylvania Colonial Penn Center, 3641 Locust Walk, Philadelphia, PA, 19104, USA.
Sci Rep. 2022 Aug 11;12(1):13658. doi: 10.1038/s41598-022-17011-7.
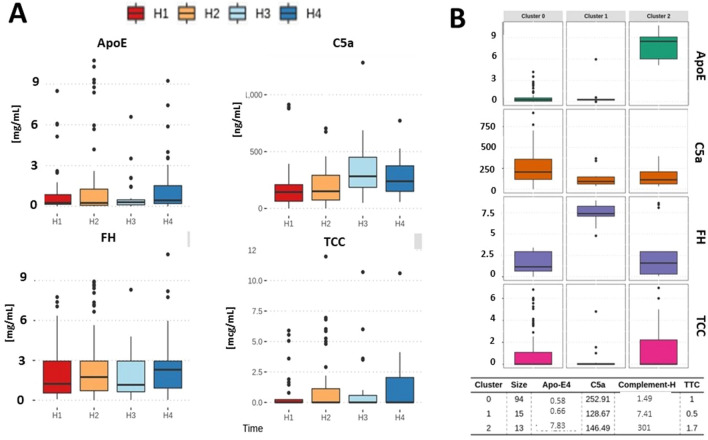
A complement effect on homeostasis during infection is determined by both cytotoxic (activate complement component 5 (C5a) terminal cytotoxic complex (TCC)), and cytoprotective elements (complement factor H (FH), as well as apolipoprotein E (ApoE)). Here, we investigated the gap in knowledge in their blood milieu during SARS-CoV-2 infection with respect to the viral burden, level of tissue necrosis, and immunological response. 101 patients hospitalized with a PCR-confirmed diagnosis of COVID-19 had blood collected at H1 (48 h), H2 (3-4 Days), H3 (5-7 days), H4 (more than 7 days up to 93 days). Pre-existing conditions, treatment, the incidence of cerebrovascular events (CVA), a history of deep venous thrombosis (DVT) and pulmonary embolism (PE), and mortality was collected using electronic medical records. Plasma C5a, TCC, FH, and ApoE were considered as a complement milieu. Tissue necrosis (HMGB1, RAGE), non-specific inflammatory responses (IL-6, C-reactive protein), overall viral burden (SARS-CoV-2 spike protein), and specific immune responses (IgG, IgA, IgM directed αS- & N-proteins) were assessed simultaneously. C5a remained elevated across all time points, with the peak at 5-7 days. Studied elements of complement coalesced around three clusters: #0 (↑↑↑C5a, ↑↑TCC, ↓↓ApoE), #1 ↑C5a, ↑TCC, ↑↑↑FH); #2 (↑C5a, ↑TCC, ↑FH, ↑↑↑ApoE). The decline in FH and ApoE was a predictor of death, while TCC and C5a correlated with patient length of stay, APACHE, and CRP. Increased levels of C5a (Δ = 122.64; p = 0.0294; data not shown) and diminished levels of FH (Δ = 836,969; p = 0.0285; data not shown) co-existed with CVA incidence. C5a correlated storngly with blood RAGE and HMGB1, but not with viral load and immunological responsiveness. Remdesivir positively affected FH preservation, while convalescent plasma treatment elevated C5a levels. Three clusters of complement activation demonstrated a various milieu of ApoE & FH vs C5a & TCC in COVID-19 patients. Complement activation is linked to increased necrosis markers but not to viral burden or immune system response.
在感染过程中,补体的内稳作用由细胞毒性(激活补体成分 5(C5a)末端细胞毒性复合物(TCC))和细胞保护元素(补体因子 H(FH)以及载脂蛋白 E(ApoE))决定。在这里,我们研究了 SARS-CoV-2 感染期间其血液环境中与病毒载量、组织坏死程度和免疫反应相关的知识空白。101 名经 PCR 确诊为 COVID-19 的住院患者在 H1(48 小时)、H2(3-4 天)、H3(5-7 天)、H4(7 天以上至 93 天)采集血液。使用电子病历收集患者的既往病史、治疗方法、脑血管事件(CVA)发生率、深静脉血栓形成(DVT)和肺栓塞(PE)病史和死亡率。血浆 C5a、TCC、FH 和 ApoE 被认为是补体环境。同时评估组织坏死(HMGB1、RAGE)、非特异性炎症反应(IL-6、C 反应蛋白)、总病毒载量(SARS-CoV-2 刺突蛋白)和特异性免疫反应(针对 αS- 和 N-蛋白的 IgG、IgA、IgM)。C5a 在所有时间点均升高,峰值出现在 5-7 天。研究的补体元素聚集在三个簇中:#0(↑↑↑C5a、↑↑TCC、↓↓ApoE)、#1 ↑C5a、↑TCC、↑↑↑FH);#2(↑C5a、↑TCC、↑FH、↑↑↑ApoE)。FH 和 ApoE 的下降是死亡的预测因素,而 TCC 和 C5a 与患者住院时间、APACHE 和 CRP 相关。C5a 水平升高(Δ=122.64;p=0.0294;未显示数据)和 FH 水平降低(Δ=836969;p=0.0285;未显示数据)与 CVA 发生率并存。C5a 与血液 RAGE 和 HMGB1 强烈相关,但与病毒载量和免疫反应性无关。瑞德西韦能有效维持 FH 的含量,而恢复期血浆治疗能升高 C5a 水平。COVID-19 患者中补体激活表现出三种不同的 ApoE & FH 与 C5a & TCC 环境。补体激活与增加的坏死标志物相关,但与病毒载量或免疫系统反应无关。