Li Tao, Dong Tiantian, Cui Yuanshan, Meng Xiangrui, Dai Zhao
Department of Anesthesiology, The Affiliated Yantai Yuhuangding Hospital of Qingdao University, Yantai, China.
Department of Urology, The Affiliated Yantai Yuhuangding Hospital of Qingdao University, Yantai, China.
Front Surg. 2022 Jul 26;9:937293. doi: 10.3389/fsurg.2022.937293. eCollection 2022.
Postoperative delirium (POD) starts in the recovery room and occurs up to 5 days after surgery. However, the POD guidelines issued by the European Society of Anesthesiology (ESA) suggest that the effect of regional anesthesia on POD is controversial. This meta-analysis aims to investigate whether perioperative regional anesthesia reduced the incidence of POD.
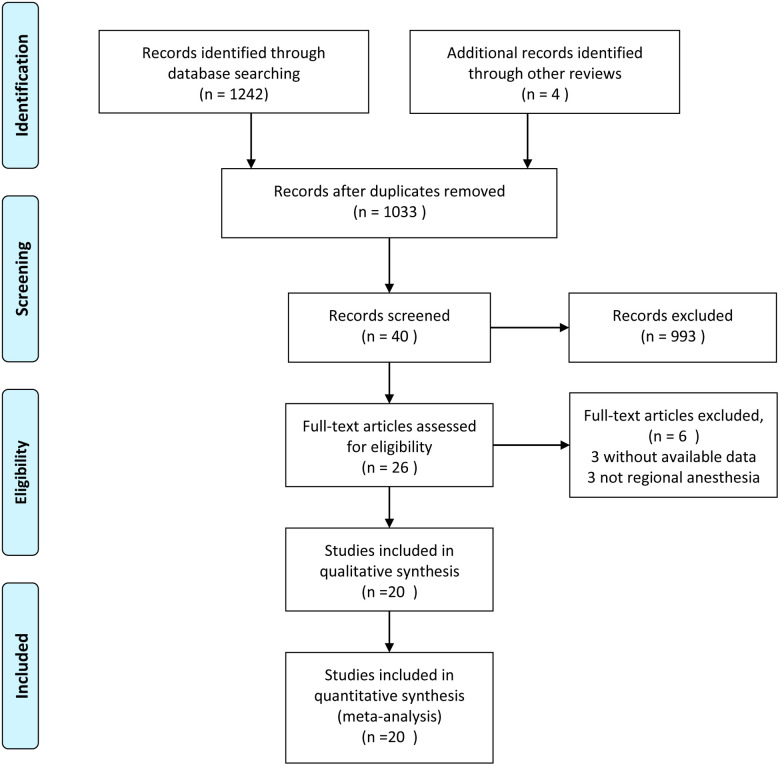
Standard Published randomized controlled trails (RCTs) were searched from bibliographic databases to identify all evidence that reported regional anesthesia assessing incident delirium following diverse surgeries. The primary outcome was the incidence of POD, and the secondary outcomes were POD scores, pain scores, and emergence time. The relative risk (RR) for dichotomous outcomes and the weighted or standardized mean difference (WMD, SMD) for continuous outcomes were estimated using a random-effects model.
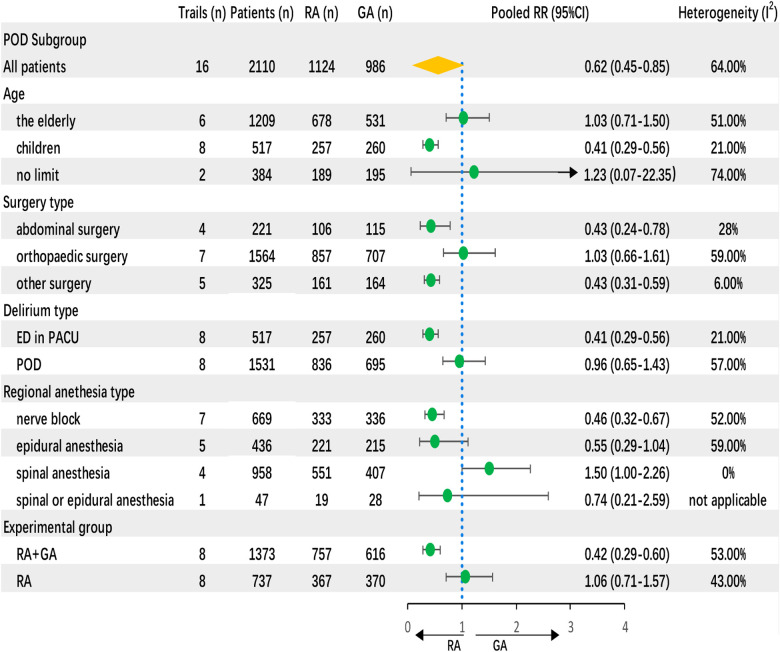
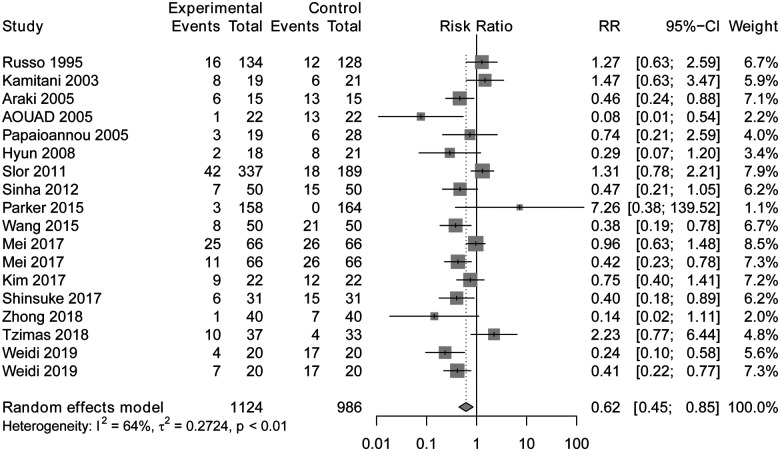
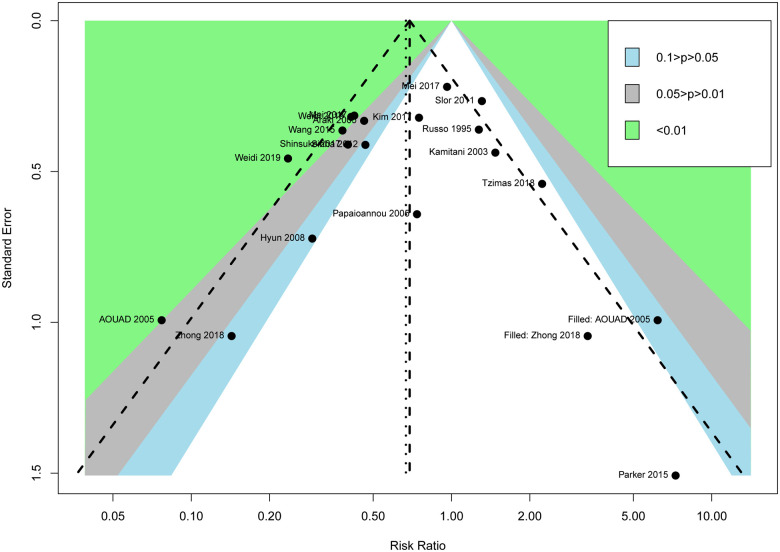
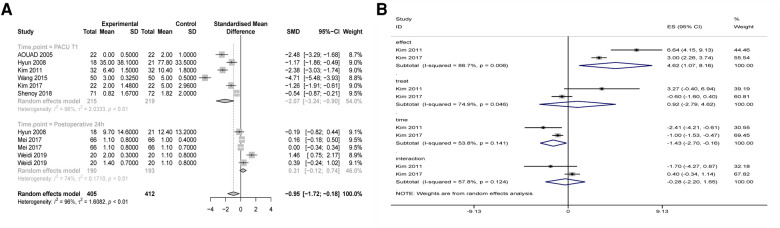
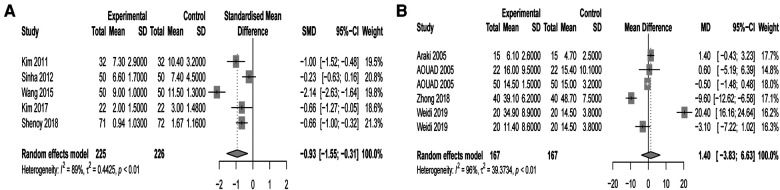
Twenty RCTs with 2110 randomized participants undergoing different surgeries were included. Meta-analysis showed that regional anesthesia was associated with less POD incidence compared to general anesthesia (total intravenous anesthesia (TIVA) or inhalation anesthesia) (relative risk (RR) = 0.62, 95% confidence interval (CI) = 0.45-0.85)). Subgroup analysis showed that the decrease in POD incidence was associated with a nerve block (0.46, 95% CI = 0.32-0.67) and regional-combined-general anesthesia (0.42, 95% CI = 0.29-0.60). Regional anesthesia significantly reduced POD incidence in the recovery room after pediatric surgeries (0.41, 95% CI = 0.29-0.56). Regional anesthesia also reduced the POD score (SMD -0.93, 95% CI = -1.55 to -0.31) and pain score (SMD -0.95, 95% CI = -1.72 to -0.81). There was no significant difference in emergence time between regional anesthesia and general anesthesia (WMD -1.40, 95% CI = -3.83 to 6.63).
There was a significant correlation between regional anesthesia and the decrease in POD incidence, POD score, and pain score.
术后谵妄(POD)始于恢复室,发生在术后长达5天内。然而,欧洲麻醉学会(ESA)发布的POD指南表明,区域麻醉对POD的影响存在争议。本荟萃分析旨在调查围手术期区域麻醉是否降低了POD的发生率。
从文献数据库中检索标准发表的随机对照试验(RCT),以识别所有报告区域麻醉评估不同手术后谵妄发生率的证据。主要结局是POD的发生率,次要结局是POD评分、疼痛评分和苏醒时间。使用随机效应模型估计二分结局的相对风险(RR)和连续结局的加权或标准化平均差(WMD,SMD)。
纳入了20项RCT,共2110名接受不同手术的随机参与者。荟萃分析表明,与全身麻醉(全静脉麻醉(TIVA)或吸入麻醉)相比,区域麻醉与较低的POD发生率相关(相对风险(RR)=0.62,95%置信区间(CI)=0.45-0.85)。亚组分析表明,POD发生率的降低与神经阻滞(0.46,95%CI=0.32-0.67)和区域联合全身麻醉(0.42,95%CI=0.29-0.60)有关。区域麻醉显著降低了小儿手术后恢复室的POD发生率(0.41,95%CI=0.29-0.56)。区域麻醉还降低了POD评分(SMD -0.93,95%CI=-1.55至-0.31)和疼痛评分(SMD -0.95,95%CI=-1.72至-0.81)。区域麻醉和全身麻醉在苏醒时间上无显著差异(WMD -1.40,95%CI=-3.83至6.63)。
区域麻醉与POD发生率、POD评分和疼痛评分的降低之间存在显著相关性。