West China Biomedical Big Data Center, West China Hospital, Sichuan University, Guo Xue Lane 37, 610041, Chengdu, China.
West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, China.
Eur J Epidemiol. 2022 Sep;37(9):947-958. doi: 10.1007/s10654-022-00898-x. Epub 2022 Aug 13.
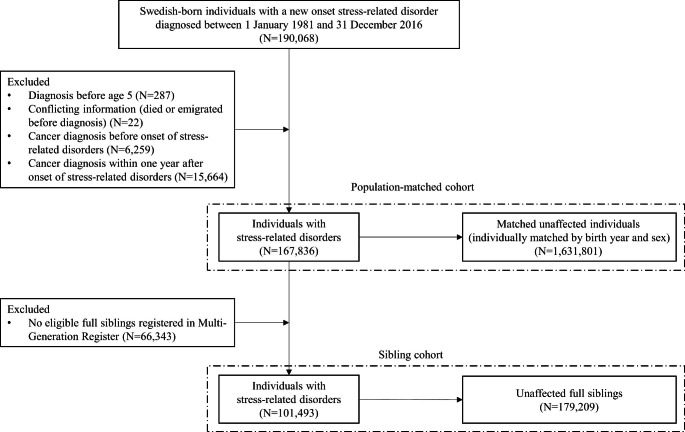
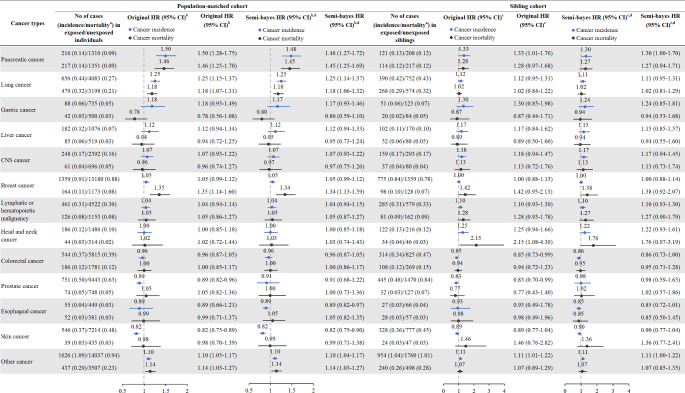
Prior research has suggested a potential role of psychological stress on cancer development while the role of familial factors on this association is underexplored. We conducted a nationwide cohort study including 167,836 individuals with a first-onset stress-related disorder (including post-traumatic stress disorder, acute stress reaction, adjustment disorder and other stress reactions) diagnosed between 1981 and 2016 in Sweden (i.e., exposed patients), 1,631,801 birth year- and sex-matched unexposed individuals, and 179,209 unaffected full siblings of the exposed patients. Cox models were used to estimate the hazard ratios (HRs) of newly diagnosed cancer and cancer-related death, beyond 1 year after diagnosis of stress-related disorders. We further examined the potential mediation roles of behavior-related morbidities in the associations of stress-related disorders with smoking or alcohol-related cancer incidence and mortality. We found modestly elevated risks of cancer incidence and mortality among exposed patients compared with matched unexposed individuals (incidence: HR = 1.03, 95% CI 1.01-1.06; mortality: HR = 1.13, 95% CI 1.07-1.18), while not when comparing with full siblings (incidence: HR = 1.03, 95% CI 0.99-1.08; mortality: HR = 1.09, 95% CI 1.00-1.19). Similarly, the suggested elevations in incidence and mortality of individual cancer sites (or groups) in the population-based comparison attenuated towards null in the between-sibling comparison. The risk elevations for smoking or alcohol-related cancers in the population-based comparison (incidence: HR = 1.18, 95% CI 1.11-1.24; mortality: HR = 1.20, 95% CI 1.12-1.29) were partially mediated by alcohol-related morbidities during follow-up. Collectively, our findings suggest that the association between stress-related disorders and cancer risk and mortality is largely explained by familial factors, including shared behavioral hazards.
先前的研究表明,心理压力可能会影响癌症的发展,而家族因素在这方面的作用尚未得到充分探索。我们进行了一项全国性的队列研究,纳入了 1981 年至 2016 年期间在瑞典首次诊断出应激相关障碍(包括创伤后应激障碍、急性应激反应、适应障碍和其他应激反应)的 167836 名患者(即暴露患者)、1631801 名按出生年份和性别匹配的未暴露个体,以及 179209 名暴露患者未受影响的全同胞。使用 Cox 模型估计应激相关障碍诊断后 1 年以上新发癌症和癌症相关死亡的风险比(HR)。我们进一步研究了行为相关疾病在应激相关障碍与吸烟或酒精相关癌症发病和死亡率之间的关联中的潜在中介作用。我们发现,与匹配的未暴露个体相比,暴露患者的癌症发病率和死亡率略高(发病率:HR=1.03,95%CI1.01-1.06;死亡率:HR=1.13,95%CI1.07-1.18),而与全同胞相比则没有(发病率:HR=1.03,95%CI0.99-1.08;死亡率:HR=1.09,95%CI1.00-1.19)。同样,在基于人群的比较中,个别癌症部位(或组)发病率和死亡率的升高在同胞间比较中趋于零。在基于人群的比较中,吸烟或酒精相关癌症的风险升高(发病率:HR=1.18,95%CI1.11-1.24;死亡率:HR=1.20,95%CI1.12-1.29)在随访期间部分由酒精相关疾病所介导。总的来说,我们的研究结果表明,应激相关障碍与癌症风险和死亡率之间的关联在很大程度上可以用家族因素来解释,包括共同的行为危险因素。