Shah Shailja C, Canakis Andrew, Halvorson Alese E, Dorn Chad, Wilson Otis, Denton Jason, Hauger Richard, Hunt Christine, Suzuki Ayako, Matheny Michael E, Siew Edward, Hung Adriana, Greevy Robert A, Roumie Christianne L
Gastroenterology Section, VA San Diego, San Diego, California.
Division of Gastroenterology, University of California, San Diego, San Diego, California.
Gastro Hep Adv. 2022;1(6):977-984. doi: 10.1016/j.gastha.2022.06.015. Epub 2022 Aug 7.
Gastrointestinal (GI) symptoms are well-recognized manifestations of coronavirus disease 2019 (COVID-19). Our primary objective was to evaluate the association between GI symptoms and COVID-19 severity.
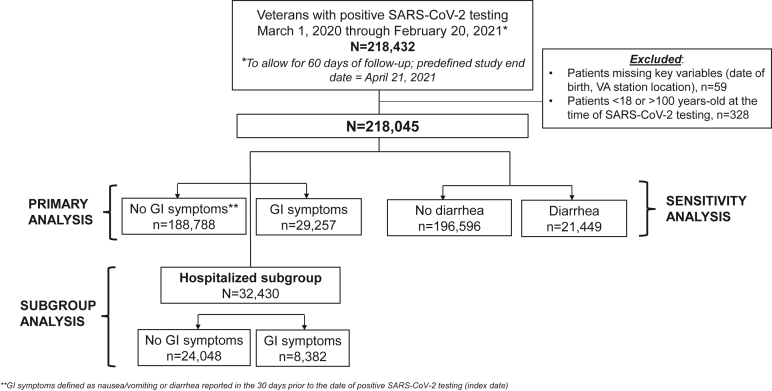
In this nationwide cohort of US veterans, we evaluated GI symptoms (nausea/vomiting/diarrhea) reported 30 days before and including the date of positive SARS-CoV-2 testing (March 1, 2020, to February 20, 2021). All patients had ≥1 year of prior baseline data and ≥60 days follow-up relative to the test date. We used propensity score (PS)-weighting to balance covariates in patients with vs without GI symptoms. The primary composite outcome was severe COVID-19, defined as hospital admission, intensive care unit admission, mechanical ventilation, or death within 60 days of positive testing.
Of 218,045 SARS-CoV-2 positive patients, 29,257 (13.4%) had GI symptoms. After PS weighting, all covariates were balanced. In the PS-weighted cohort, patients with vs without GI symptoms had severe COVID-19 more often (29.0% vs 17.1%; < .001). When restricted to hospitalized patients (14.9%; n=32,430), patients with GI symptoms had similar frequencies of intensive care unit admission and mechanical ventilation compared with patients without symptoms. There was a significant age interaction; among hospitalized patients aged ≥70 years, lower COVID-19-associated mortality was observed in patients with vs without GI symptoms, even after accounting for COVID-19-specific medical treatments.
In the largest integrated US health care system, SARS-CoV-2-positive patients with GI symptoms experienced severe COVID-19 outcomes more often than those without symptoms. Additional research on COVID-19-associated GI symptoms may inform preventive efforts and interventions to reduce severe COVID-19.
胃肠道(GI)症状是2019冠状病毒病(COVID-19)的公认表现。我们的主要目标是评估GI症状与COVID-19严重程度之间的关联。
在这个美国退伍军人的全国性队列中,我们评估了在严重急性呼吸综合征冠状病毒2检测呈阳性日期(2020年3月1日至2021年2月20日)之前30天内报告的GI症状(恶心/呕吐/腹泻),包括该日期。所有患者相对于检测日期有≥1年的既往基线数据和≥60天的随访。我们使用倾向评分(PS)加权来平衡有或没有GI症状患者的协变量。主要复合结局是严重COVID-19,定义为在检测呈阳性后60天内住院、入住重症监护病房、机械通气或死亡。
在218,045例严重急性呼吸综合征冠状病毒2阳性患者中,29,257例(13.4%)有GI症状。经过PS加权后,所有协变量均得到平衡。在PS加权队列中,有GI症状的患者比没有GI症状的患者更常出现严重COVID-19(29.0%对17.1%;P<0.001)。当仅限于住院患者(14.9%;n=32,430)时,有GI症状的患者与无症状患者相比,入住重症监护病房和机械通气的频率相似。存在显著的年龄交互作用;在≥70岁的住院患者中,即使在考虑了COVID-19特异性医疗治疗后,有GI症状的患者与没有GI症状的患者相比,COVID-19相关死亡率更低。
在最大的美国综合医疗保健系统中,有GI症状的严重急性呼吸综合征冠状病毒2阳性患者比无症状患者更常出现严重COVID-19结局。对COVID-19相关GI症状的进一步研究可能为减少严重COVID-19的预防措施和干预提供信息。