Stewart Darren E, Foutz Julia, Kamal Layla, Weiss Samantha, McGehee Harrison S, Cooper Matthew, Gupta Gaurav
Research Department, United Network for Organ Sharing, Richmond, Virginia, USA.
Division of Nephrology, School of Medicine, Virginia Commonwealth University, Richmond, Virginia, USA.
Kidney Int Rep. 2022 May 30;7(8):1850-1865. doi: 10.1016/j.ekir.2022.05.027. eCollection 2022 Aug.
The role of procurement biopsies in deceased donor kidney evaluation is debated in light of uncertainty about the influence of biopsy findings on recipient outcomes. The literature is filled with conflicting and ambiguous findings typically derived from small studies focused on short-term outcomes or reliant on biopsies prepared by methods impractical in the time-sensitive context of organ procurement.
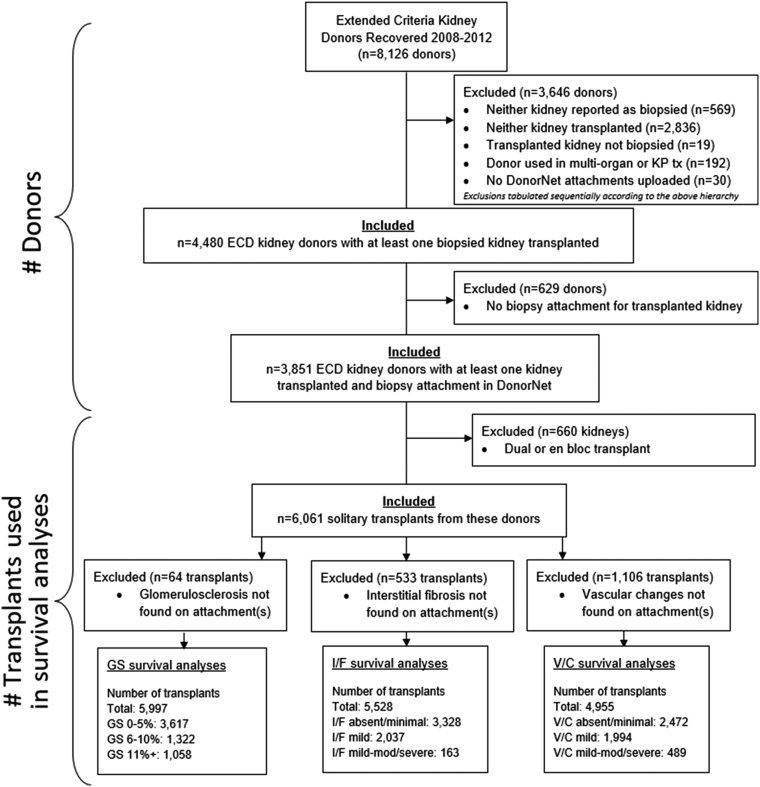
After manual data entry of DonorNet attachments from 4480 extended criteria donors (ECDs) recovered in the United States from 2008 to 2012, we applied causal inference methods in a Cox regression framework to estimate independent effects of glomerulosclerosis (GS), interstitial fibrosis, and vascular changes on long-term kidney graft survival. Kidney discard rates from 2018 to 2019 were evaluated to characterize contemporary kidney utilization patterns.
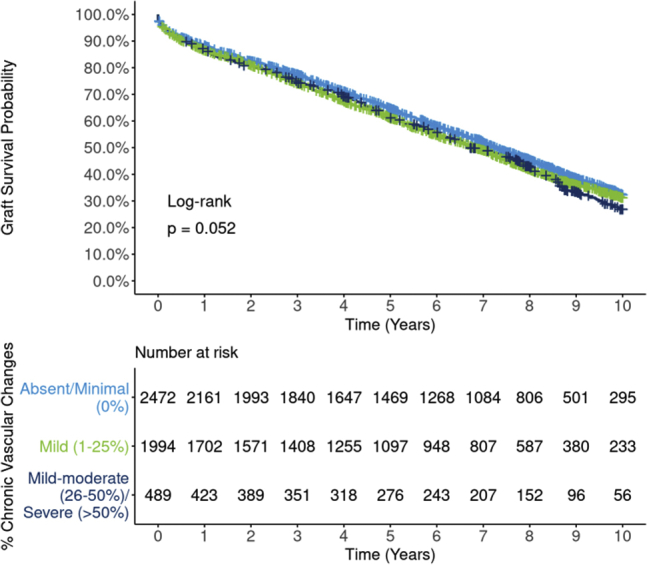
Effects of interstitial fibrosis and vascular changes were largely attenuated after adjusting for potentially confounding donor and recipient variables, although conclusions are less certain for severe levels due to smaller sample sizes. By contrast, significant effects of GS (>10% vs. 0%-5%) persisted even after adjustment (all-cause, hazard ratio [HR] 1.18; 95% CI 1.06, 1.28; death-censored, HR 1.28; 95% CI 1.08, 1.46) but plateaued beyond 10%. By contrast, kidney discard rates increased precipitously as GS rose >10%.
Despite being obtained under less than ideal conditions, estimated GS from a procurement biopsy is independently associated with long-term graft survival, above and beyond standard clinical parameters, in ECD transplants. However, the disproportionately high likelihood of discard for kidneys with GS >10% is unjustified. The outsized effect of GS on kidney utilization should be tempered and commensurate with its effect on outcomes.
鉴于活检结果对受体预后影响的不确定性,尸肾评估中获取活检标本的作用存在争议。文献中充斥着相互矛盾且含糊不清的研究结果,这些结果通常来自于聚焦短期预后的小型研究,或者依赖于在器官获取的时间敏感背景下不实用的方法制备的活检标本。
在手动录入2008年至2012年在美国获取的4480例扩大标准供体(ECD)的DonorNet附件数据后,我们在Cox回归框架中应用因果推断方法,以估计肾小球硬化(GS)、间质纤维化和血管变化对肾移植长期存活的独立影响。评估了2018年至2019年的肾脏丢弃率,以描述当代肾脏利用模式。
在调整了可能混淆的供体和受体变量后,间质纤维化和血管变化的影响大多减弱,尽管由于样本量较小,对于严重程度的结论不太确定。相比之下,即使在调整后,GS(>10% vs. 0%-5%)的显著影响仍然存在(全因死亡,风险比[HR] 1.18;95%可信区间1.06,1.28;死亡删失,HR 1.28;95%可信区间1.08,1.46),但在超过10%后趋于平稳。相比之下,随着GS升高>10%,肾脏丢弃率急剧上升。
尽管是在不太理想的条件下获得的,但在ECD移植中,从获取的活检标本估计的GS独立于标准临床参数与长期移植存活相关。然而,GS>10%的肾脏丢弃可能性过高是不合理的。GS对肾脏利用的过大影响应得到缓和,并与其对预后的影响相称。