Savitska Daria, Hess Morgan, Calis Dila, Marchetta Philine, Harasztosi Csaba, Fink Stefan, Eckert Philipp, Ruth Peter, Rüttiger Lukas, Knipper Marlies, Singer Wibke
Department of Otolaryngology, Head and Neck Surgery, Tübingen Hearing Research Centre, Molecular Physiology of Hearing, University of Tübingen, Tübingen, Germany.
Department of Pharmacology, Toxicology and Clinical Pharmacy, Institute of Pharmacy, University of Tübingen, Tübingen, Germany.
Front Neurosci. 2022 Jul 29;16:864706. doi: 10.3389/fnins.2022.864706. eCollection 2022.
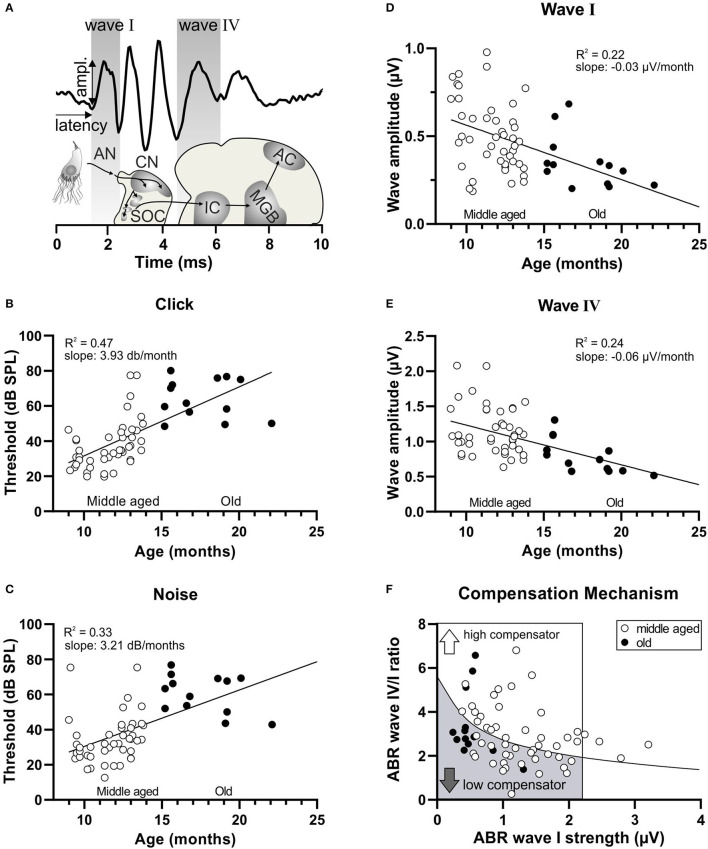
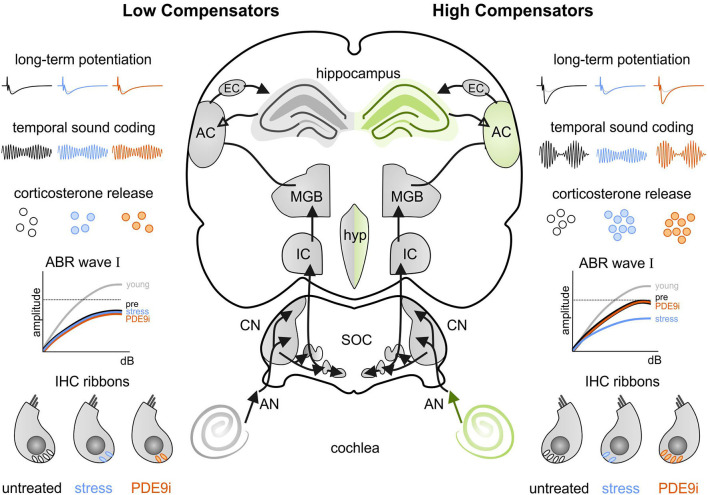
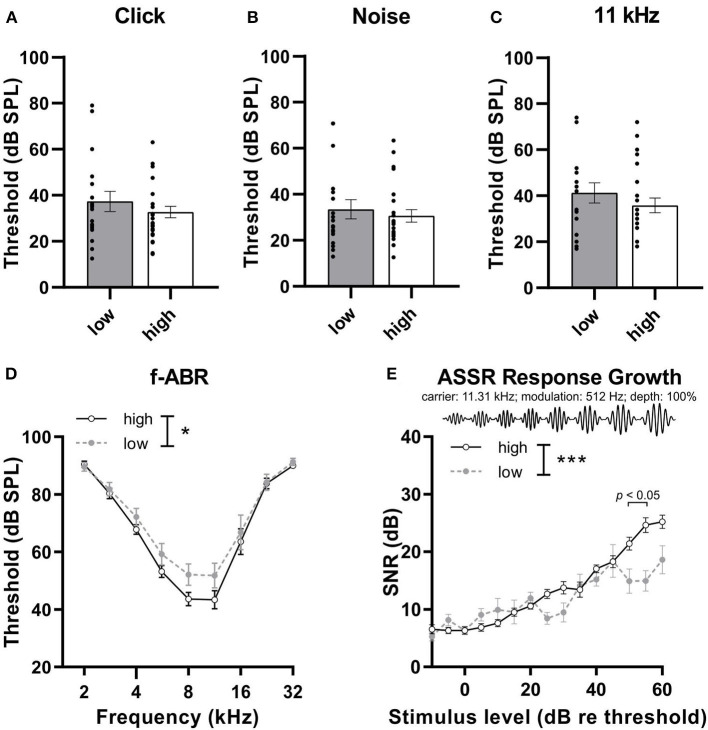
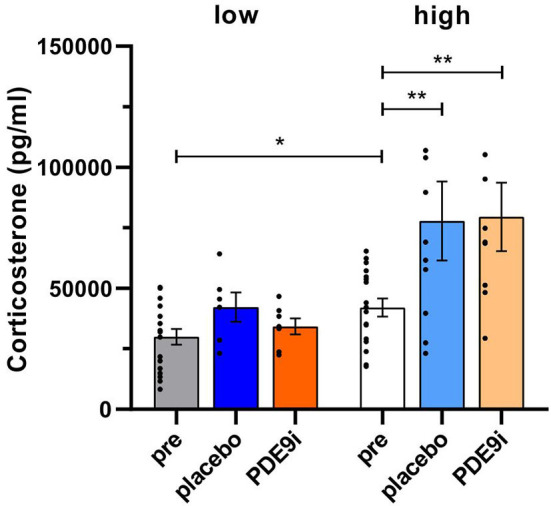
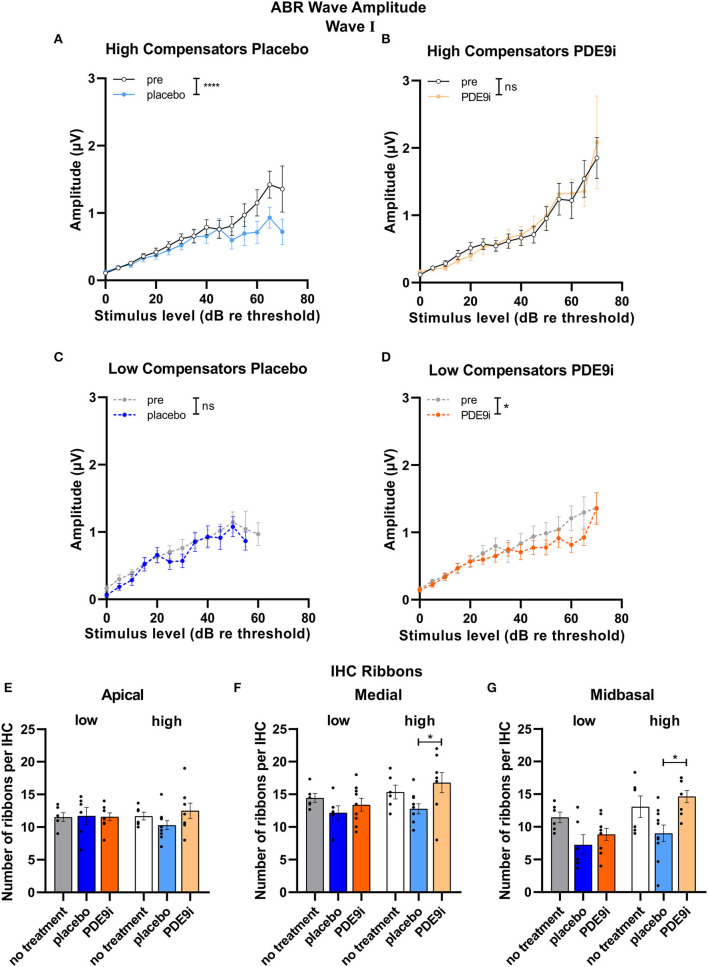
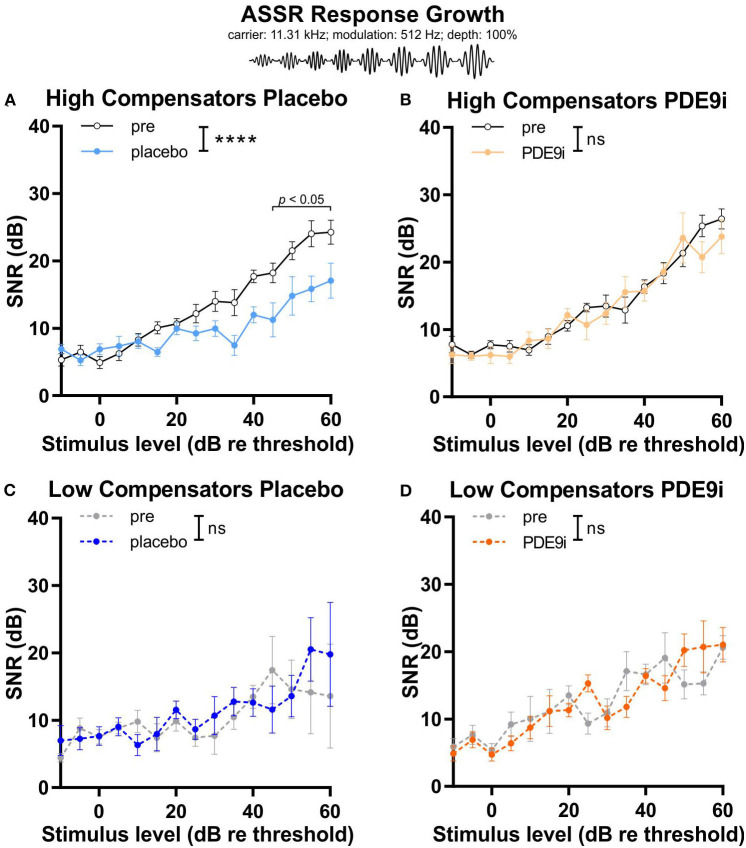
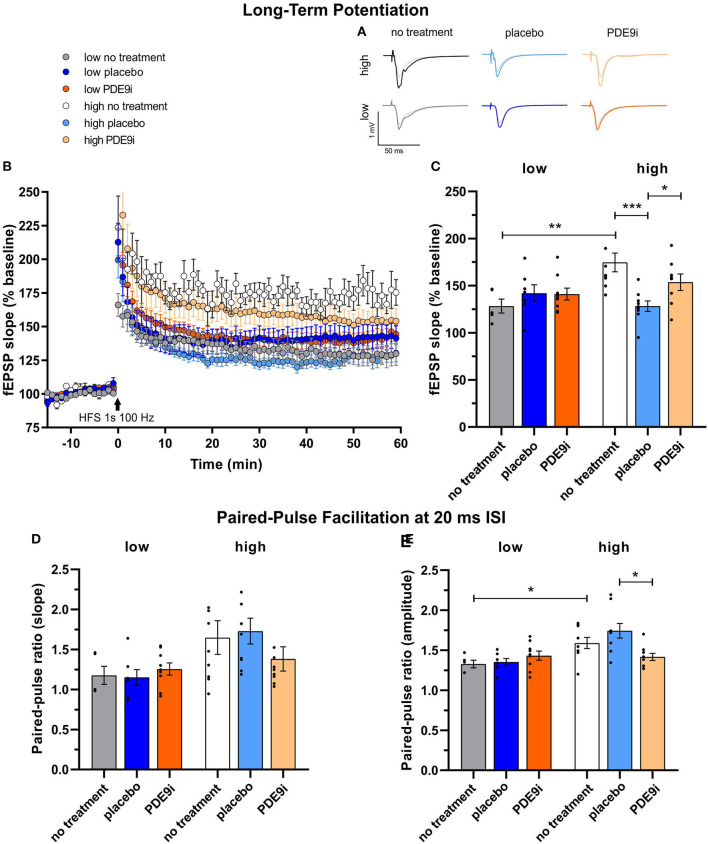
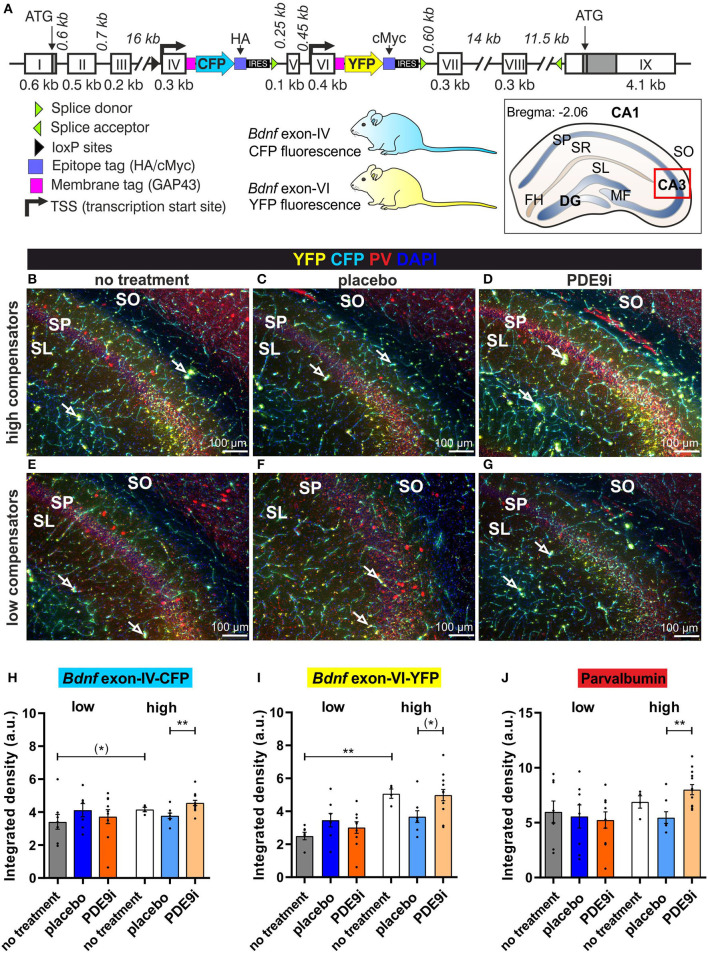
In light of the increasing evidence supporting a link between hearing loss and dementia, it is critical to gain a better understanding of the nature of this relationship. We have previously observed that following cochlear synaptopathy, the temporal auditory processing (e.g., auditory steady state responses, ASSRs), is sustained when reduced auditory input is centrally compensated. This central compensation process was linked to elevated hippocampal long-term potentiation (LTP). We further observed that, independently of age, central responsiveness to cochlear synaptopathy can differ, resulting in either a low or high capacity to compensate for the reduced auditory input. Lower central compensation resulted in poorer temporal auditory processing, reduced hippocampal LTP, and decreased recruitment of activity-dependent brain-derived neurotrophic factor (BDNF) expression in hippocampal regions (). Higher central compensation capacity resulted in better temporal auditory processing, higher LTP responses, and increased activity-dependent BDNF expression in hippocampal regions. Here, we aimed to identify modifying factors that are potentially responsible for these different central responses. Strikingly, a poorer central compensation capacity was linked to lower corticosterone levels in comparison to those of . responded to repeated placebo injections with elevated blood corticosterone levels, reduced auditory brainstem response (ABR) wave I amplitude, reduced inner hair cell (IHC) ribbon number, diminished temporal processing, reduced LTP responses, and decreased activity-dependent hippocampal BDNF expression. In contrast, the same stress exposure through injection did not elevate blood corticosterone levels in , nor did it reduce IHC ribbons, ABR wave I amplitude, ASSR, LTP, or BDNF expression as seen in . Interestingly, in , the stress-induced responses, such as a decline in ABR wave I amplitude, ASSR, LTP, and BDNF could be restored through the "memory-enhancing" drug phosphodiesterase 9A inhibitor (PDE9i). In contrast, the same treatment did not improve these aspects in . Thus, central compensation of age-dependent cochlear synaptopathy is a glucocorticoid and cyclic guanosine-monophosphate (cGMP)-dependent neuronal mechanism that fails upon a blunted stress response.
鉴于越来越多的证据支持听力损失与痴呆症之间存在联系,更深入地了解这种关系的本质至关重要。我们之前观察到,在耳蜗突触病变后,当减少的听觉输入在中枢得到补偿时,颞叶听觉处理(如听觉稳态反应,ASSRs)得以维持。这种中枢补偿过程与海马体长期增强(LTP)升高有关。我们进一步观察到,与年龄无关,中枢对耳蜗突触病变的反应性可能不同,导致对减少的听觉输入的补偿能力有高有低。较低的中枢补偿导致较差的颞叶听觉处理、海马体LTP降低以及海马体区域中活性依赖性脑源性神经营养因子(BDNF)表达的募集减少。较高的中枢补偿能力导致更好的颞叶听觉处理、更高的LTP反应以及海马体区域中活性依赖性BDNF表达增加。在此,我们旨在确定可能导致这些不同中枢反应的调节因素。令人惊讶的是,与……相比,较差的中枢补偿能力与较低的皮质酮水平有关。……对重复的安慰剂注射的反应是血液皮质酮水平升高、听觉脑干反应(ABR)波I振幅降低、内毛细胞(IHC)带状小体数量减少、颞叶处理能力下降、LTP反应降低以及海马体中活性依赖性BDNF表达减少。相比之下,通过注射进行的相同应激暴露在……中并未升高血液皮质酮水平,也未像在……中那样降低IHC带状小体、ABR波I振幅、ASSR、LTP或BDNF表达。有趣的是,在……中,应激诱导的反应,如ABR波I振幅、ASSR、LTP和BDNF的下降,可以通过“增强记忆”药物磷酸二酯酶9A抑制剂(PDE9i)恢复。相比之下,相同的治疗在……中并未改善这些方面。因此,年龄依赖性耳蜗突触病变的中枢补偿是一种糖皮质激素和环磷酸鸟苷(cGMP)依赖性神经元机制,在应激反应减弱时会失效。