Tanimoto Terutaka, Noda Takuo, Imaji Reisuke, Nouso Hiroshi
Department of Pediatric Surgery, Okayama University Hospital, 2-5-1 Shikatacho, Kita-ku, Okayama, Okayama, 700-8558, Japan.
Department of Pediatric Surgery, Hiroshima City Hiroshima Citizens Hospital, 7-33 Motomachi, Naka-ku, Hiroshima, Hiroshima, 730-8518, Japan.
Surg Case Rep. 2022 Aug 15;8(1):156. doi: 10.1186/s40792-022-01513-7.
Esophageal atresia with or without a trachea-esophageal fistula occurs due to the failure of separation or incomplete development of the foregut. Therefore, esophageal atresia is often associated with various forms of tracheobronchial anomalies. We report an extremely rare case of esophageal atresia.
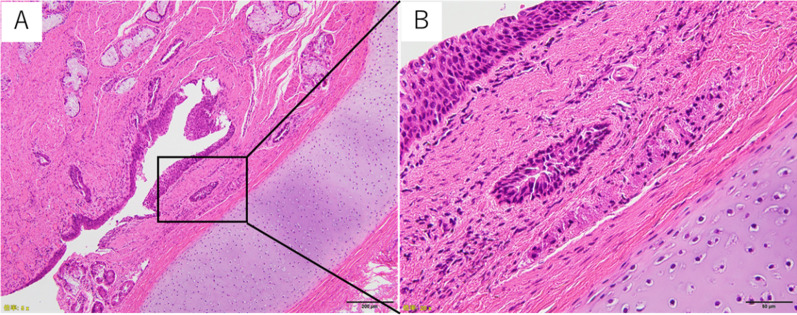
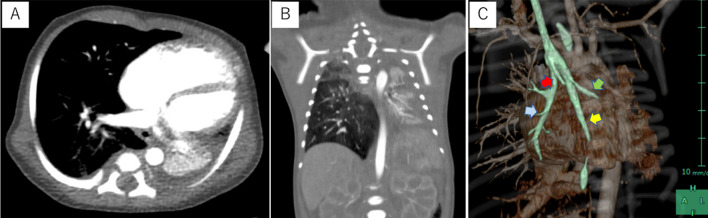
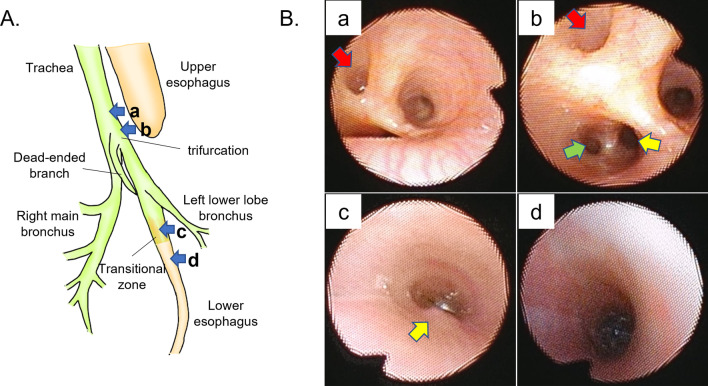
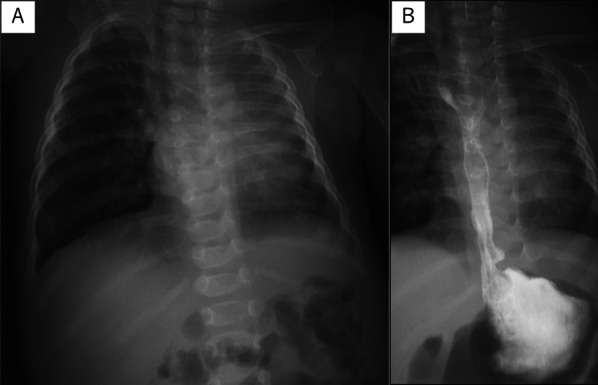
A female infant was born at 37 weeks of gestation and weighed 2596 g. A diagnosis of esophageal atresia and total anomalous pulmonary vein return type III were confirmed. The infant had respiratory distress that required tracheal intubation and ventilatory support soon after birth. Temporary banding of the gastroesophageal junction and gastrostomy were performed on the second day of life. However, her respiratory condition deteriorated due to atelectasis of the left lung and compensatory hyperinflation of the right lung. Preoperative examinations showed the unilobe and atelectatic left lung. The trachea was trifurcated in three directions, and the branch that was expected to be the left main bronchus was blind-ended. The dorsal branch was cartilaginous and bifurcated into the left lower lobe bronchus and lower esophagus approximately 1 cm distal from the tracheal trifurcation. The cartilaginous tissue continued to the lower esophagus. The diagnosis of esophageal atresia with the lower esophagus which originated from the left lower lobe bronchus was made. Esophageal atresia repair was performed when the patient was 4 months of age. The esophagus was dissected distally to the bifurcation of the left lower lobe bronchus via right thoracotomy. The lower esophagus was bronchial-like in appearance, transitioning to the normal esophageal wall approximately 7 mm distal to the transected edge. The cartilage tissue was completely resected during surgery, and a primary end-to-end anastomosis of the esophagus was successfully performed. Histopathological findings revealed that the extracted specimen was surrounded by tracheal cartilage and that the inner surface was covered by stratified squamous epithelium that originated from the esophagus.
In cases of esophageal atresia with an atypical clinical presentation, there may be unique structural abnormalities of the foregut. We emphasize the importance of a preoperative surgical planning since an inadequate operation can lead to fatal complications.
食管闭锁伴或不伴气管食管瘘是由于前肠分离失败或发育不完全所致。因此,食管闭锁常伴有各种形式的气管支气管异常。我们报告一例极其罕见的食管闭锁病例。
一名女婴在妊娠37周时出生,体重2596克。确诊为食管闭锁和III型完全性肺静脉异位引流。婴儿出生后不久即出现呼吸窘迫,需要气管插管和通气支持。出生后第二天进行了胃食管交界处临时束带术和胃造瘘术。然而,由于左肺肺不张和右肺代偿性过度充气,她的呼吸状况恶化。术前检查显示左肺单叶且肺不张。气管向三个方向分叉,预期为左主支气管的分支呈盲端。背侧分支为软骨性,在气管分叉处远端约1厘米处分为左下叶支气管和下食管。软骨组织延续至下食管。诊断为食管闭锁,其下食管起源于左下叶支气管。患儿4个月大时进行了食管闭锁修复术。通过右胸切开术将食管向远端解剖至左下叶支气管分叉处。下食管外观类似支气管,在横断边缘远端约7毫米处过渡为正常食管壁。手术中完全切除了软骨组织,并成功进行了食管端端吻合术。组织病理学检查结果显示,取出的标本被气管软骨包围,内表面覆盖有起源于食管的复层鳞状上皮。
在食管闭锁临床表现不典型的病例中,前肠可能存在独特的结构异常。我们强调术前手术规划的重要性,因为手术操作不当可能导致致命并发症。