Cadegiani Flavio A
Clinical Endocrinology, Corpometria Institute, Brasilia, BRA.
Clinical Endocrinology, Applied Biology, Inc., Irvine, USA.
Cureus. 2022 Aug 11;14(8):e27883. doi: 10.7759/cureus.27883. eCollection 2022 Aug.
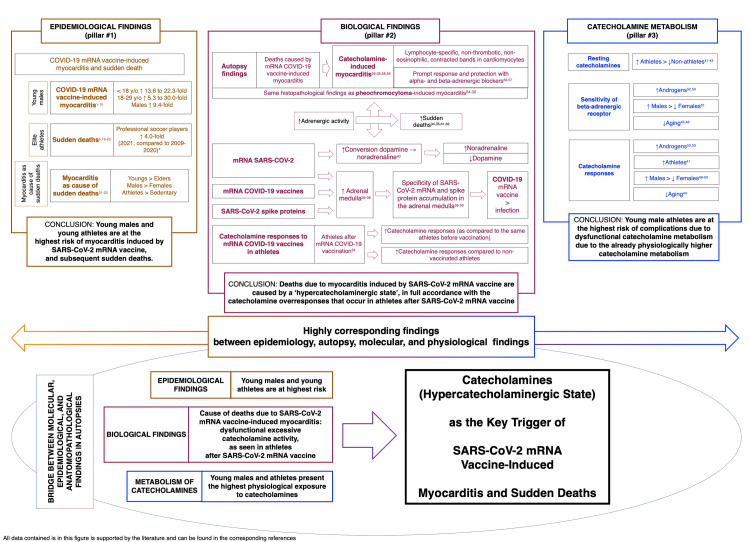
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) mRNA vaccine-induced myocarditis is a rare but well-documented complication in young males. The increased incidence of sudden death among athletes following vaccination has been reported and requires further investigation. Whether the risk of myocarditis, a known major cause of sudden death in young male athletes, also increases after coronavirus disease 2019 (COVID-19) infection is unknown. The severity and implications of these critical adverse effects require a thorough analysis to elucidate their key triggering mechanisms. The present review aimed to evaluate whether there is a justification to hypothesize that catecholamines in a "hypercatecholaminergic" state are the key trigger of SARS-CoV-2 mRNA vaccine-induced myocarditis and related outcomes and whether similar risks are also present following COVID-19 infection. A thorough, structured scoping review of the literature was performed to build the hypothesis through three pillars: detection of myocarditis risk, potential alterations and abnormalities identified after SARS-CoV-2 mRNA vaccination or COVID-19 infection and consequent events, and physiological characteristics of the most affected population. The following terms were searched in indexed and non-indexed peer review articles and recent preprints (<12 months): agent, "SARS-CoV-2" or "COVID-19"; event, "myocarditis" or "sudden death(s)" or "myocarditis+sudden death(s)" or "cardiac event(s)"; underlying cause, "mRNA" or "spike protein" or "infection" or "vaccine"; proposed trigger, "catecholamine(s)" or "adrenaline" or "epinephrine" or "noradrenaline" or "norepinephrine" or "testosterone"; and affected population, "young male(s)" or "athlete(s)." The rationale and data that supported the hypothesis were as follows: SARS-CoV-2 mRNA vaccine-induced myocarditis primarily affected young males, while the risk was not observed following COVID-19 infection; independent autopsies or biopsies of patients who presented post-SARS-CoV-2 mRNA vaccine myocarditis in different geographical regions enabled the conclusion that a primary hypercatecholaminergic state was the key trigger of these events; SARS-CoV-2 mRNA was densely present, and SARS-CoV-2 spike protein was progressively produced in adrenal medulla chromaffin cells, which are responsible for catecholamine production; the dihydroxyphenylalanine decarboxylase enzyme that converts dopamine into noradrenaline was overexpressed in the presence of SARS-CoV-2 mRNA, leading to enhanced noradrenaline activity; catecholamine responses were physiologically higher in young adults and males than in other populations; catecholamine responses and resting catecholamine production were higher in male athletes than in non-athletes; catecholamine responses to stress and its sensitivity were enhanced in the presence of androgens; and catecholamine expressions in young male athletes were already high at baseline, were higher following vaccination, and were higher than those in non-vaccinated athletes. The epidemiological, autopsy, molecular, and physiological findings unanimously and strongly suggest that a hypercatecholaminergic state is the critical trigger of the rare cases of myocarditis due to components from SARS-CoV-2, potentially increasing sudden deaths among elite male athletes.
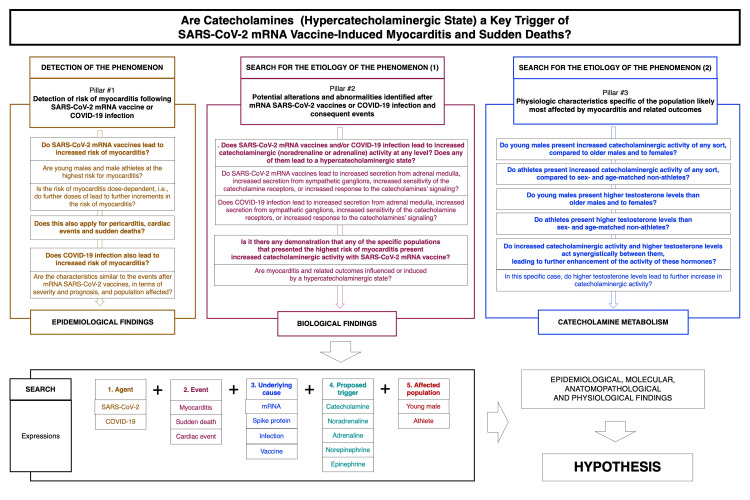
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)信使核糖核酸(mRNA)疫苗诱发的心肌炎是年轻男性中一种罕见但记录充分的并发症。据报道,接种疫苗后运动员猝死的发生率有所增加,这需要进一步调查。2019冠状病毒病(COVID-19)感染后,作为年轻男性运动员猝死已知主要原因的心肌炎风险是否也会增加尚不清楚。这些严重不良反应的严重程度和影响需要进行全面分析,以阐明其关键触发机制。本综述旨在评估是否有理由假设处于“高儿茶酚胺能”状态的儿茶酚胺是SARS-CoV-2 mRNA疫苗诱发心肌炎及相关后果的关键触发因素,以及COVID-19感染后是否也存在类似风险。通过对文献进行全面、结构化的范围综述,通过三个支柱构建这一假设:心肌炎风险的检测、SARS-CoV-2 mRNA疫苗接种或COVID-19感染后及相应事件后发现的潜在改变和异常,以及受影响最严重人群的生理特征。在索引和非索引同行评议文章以及近期预印本(<12个月)中搜索了以下术语:病原体,“SARS-CoV-2”或“COVID-19”;事件,“心肌炎”或“猝死”或“心肌炎+猝死”或“心脏事件”;潜在病因,“mRNA”或“刺突蛋白”或“感染”或“疫苗”;提出的触发因素,“儿茶酚胺”或“肾上腺素”或“肾上腺素”或“去甲肾上腺素”或“去甲肾上腺素”或“睾酮”;以及受影响人群,“年轻男性”或“运动员”。支持该假设的基本原理和数据如下:SARS-CoV-2 mRNA疫苗诱发的心肌炎主要影响年轻男性,而COVID-19感染后未观察到这种风险;对不同地理区域出现SARS-CoV-2 mRNA疫苗接种后心肌炎的患者进行独立尸检或活检后得出结论,原发性高儿茶酚胺能状态是这些事件的关键触发因素;SARS-CoV-2 mRNA大量存在,SARS-CoV-2刺突蛋白在负责儿茶酚胺产生的肾上腺髓质嗜铬细胞中逐渐产生;在存在SARS-CoV-2 mRNA的情况下,将多巴胺转化为去甲肾上腺素的二羟基苯丙氨酸脱羧酶过度表达,导致去甲肾上腺素活性增强;年轻人和男性的儿茶酚胺生理反应高于其他人群;男性运动员的儿茶酚胺反应和静息儿茶酚胺产生高于非运动员;在雄激素存在的情况下,儿茶酚胺对应激的反应及其敏感性增强;年轻男性运动员的儿茶酚胺表达在基线时就已经很高,接种疫苗后更高,且高于未接种疫苗的运动员。流行病学、尸检、分子和生理学研究结果一致且有力地表明,高儿茶酚胺能状态是SARS-CoV-2成分导致罕见心肌炎病例的关键触发因素,可能会增加精英男性运动员的猝死率。