Department of Anesthesiology, First Affiliated Hospital of Nanchang University, NO. 17, Yongwaizheng Street, Nanchang, Jiangxi, 330006, China.
Department of Anesthesiology, Shaoxing People's Hospital (Shaoxing Hospital, Zhejiang University School of Medicine), NO.568, North Zhongxing Road, Shaoxing, Zhejiang, China.
BMC Anesthesiol. 2022 Aug 16;22(1):261. doi: 10.1186/s12871-022-01798-z.
The majority of patients may experience atelectasis under general anesthesia, and the Trendelenburg position and pneumoperitoneum can aggravate atelectasis during laparoscopic surgery, which promotes postoperative pulmonary complications. Lung recruitment manoeuvres have been proven to reduce perioperative atelectasis, but it remains controversial which method is optimal. Ultrasonic imaging can be conducive to confirming the effect of lung recruitment manoeuvres. The purpose of our study was to assess the effects of ultrasound-guided alveolar recruitment manoeuvres by ultrasonography on reducing perioperative atelectasis and to check whether the effects of recruitment manoeuvres under ultrasound guidance (visual and semiquantitative) on atelectasis are superior to sustained inflation recruitment manoeuvres (classical and widely used) in laparoscopic gynaecological surgery.
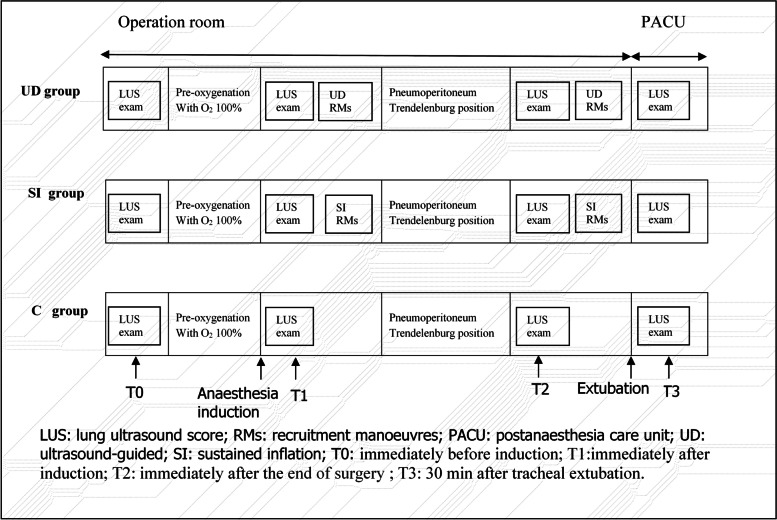
In this randomized, controlled, double-blinded study, women undergoing laparoscopic gynecological surgery were enrolled. Patients were randomly assigned to receive either lung ultrasound-guided alveolar recruitment manoeuvres (UD group), sustained inflation alveolar recruitment manoeuvres (SI group), or no RMs (C group) using a computer-generated table of random numbers. Lung ultrasonography was performed at four predefined time points. The primary outcome was the difference in lung ultrasound score (LUS) among groups at the end of surgery.
Lung ultrasound scores in the UD group were significantly lower than those in both the SI group and the C group immediately after the end of surgery (7.67 ± 1.15 versus 9.70 ± 102, difference, -2.03 [95% confidence interval, -2.77 to -1.29], P < 0.001; 7.67 ± 1.15 versus 11.73 ± 1.96, difference, -4.07 [95% confidence interval, -4.81 to -3.33], P < 0.001;, respectively). The intergroup differences were sustained until 30 min after tracheal extubation (9.33 ± 0.96 versus 11.13 ± 0.97, difference, -1.80 [95% confidence interval, -2.42 to -1.18], P < 0.001; 9.33 ± 0.96 versus 10.77 ± 1.57, difference, -1.43 [95% confidence interval, -2.05 to -0.82], P < 0.001;, respectively). The SI group had a significantly lower LUS than the C group at the end of surgery (9.70 ± 1.02 versus 11.73 ± 1.96, difference, -2.03 [95% confidence interval, -2.77 to -1.29] P < 0.001), but the benefit did not persist 30 min after tracheal extubation.
During general anesthesia, ultrasound-guided recruitment manoeuvres can reduce perioperative aeration loss and improve oxygenation. Furthermore, these effects of ultrasound-guided recruitment manoeuvres on atelectasis are superior to sustained inflation recruitment manoeuvres.
Chictr.org.cn, ChiCTR2100042731, Registered 27 January 2021, www.chictr.org.cn .
大多数患者在全身麻醉下可能会出现肺不张,而在腹腔镜手术中,头高脚低位和人工气腹会加重肺不张,从而促进术后肺部并发症。肺复张手法已被证明可以减少围手术期肺不张,但哪种方法最佳仍存在争议。超声成像有助于证实肺复张手法的效果。本研究的目的是评估超声引导下的肺泡复张手法(通过超声)对减少围手术期肺不张的作用,并检查超声引导下的复张手法(视觉和半定量)对肺不张的效果是否优于持续充气复张手法(经典且广泛应用)在腹腔镜妇科手术中的作用。
在这项随机、对照、双盲研究中,纳入了接受腹腔镜妇科手术的女性患者。患者被随机分配接受肺超声引导下的肺泡复张手法(UD 组)、持续充气肺泡复张手法(SI 组)或不接受 RM(C 组),使用计算机生成的随机数表。在四个预设时间点进行肺部超声检查。主要结局是手术结束时各组间肺超声评分(LUS)的差异。
UD 组的肺部超声评分明显低于 SI 组和 C 组,术后即刻(7.67±1.15 与 9.70±102,差异,-2.03[95%置信区间,-2.77 至-1.29],P<0.001;7.67±1.15 与 11.73±1.96,差异,-4.07[95%置信区间,-4.81 至-3.33],P<0.001,分别)。这种组间差异持续到气管拔管后 30 分钟(9.33±0.96 与 11.13±0.97,差异,-1.80[95%置信区间,-2.42 至-1.18],P<0.001;9.33±0.96 与 10.77±1.57,差异,-1.43[95%置信区间,-2.05 至-0.82],P<0.001,分别)。SI 组在手术结束时的 LUS 明显低于 C 组(9.70±1.02 与 11.73±1.96,差异,-2.03[95%置信区间,-2.77 至-1.29],P<0.001),但在气管拔管后 30 分钟时,这种获益不再持续。
全身麻醉期间,超声引导下的复张手法可以减少围手术期通气损失并改善氧合。此外,超声引导下复张手法对肺不张的作用优于持续充气复张手法。
Chictr.org.cn,ChiCTR2100042731,注册于 2021 年 1 月 27 日,www.chictr.org.cn。