Department of Clinical Science, Intervention and Technology, Division of Paediatrics, Karolinska Institutet, Stockholm, Sweden.
Department of Paediatric Nephrology, Karolinska University Hospital, Stockholm, Sweden.
Pediatr Nephrol. 2023 Apr;38(4):1205-1214. doi: 10.1007/s00467-022-05705-z. Epub 2022 Aug 17.
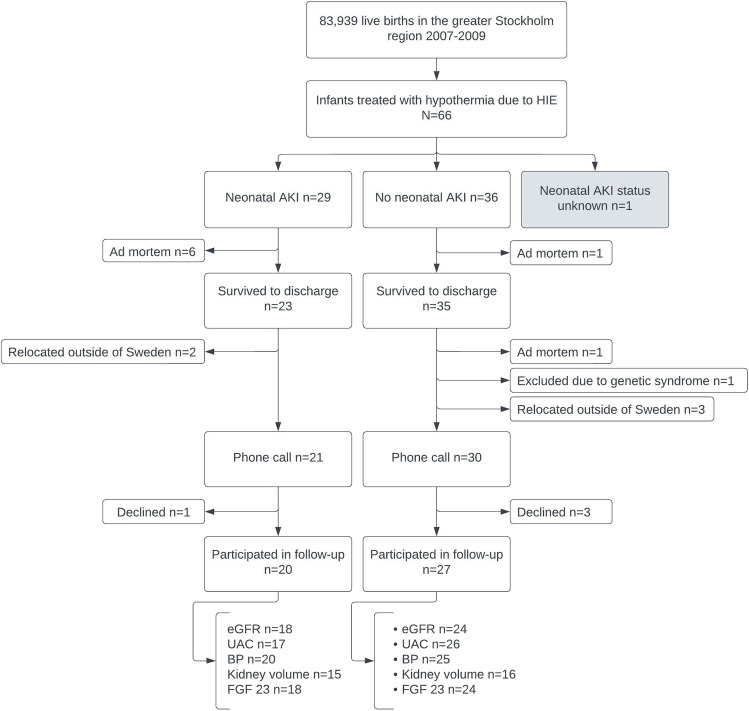
Acute kidney injury (AKI) remains common among infants with hypothermia-treated hypoxic-ischaemic encephalopathy (HIE). Little is known about long-term kidney outcomes following hypothermia treatment. We recently reported that 21% of survivors of hypothermia-treated HIE had decreased estimated glomerular filtration rate (eGFR) based on plasma creatinine in early adolescence. Here, we assessed kidney functions more comprehensively in our population-based cohort of children born in Stockholm 2007-2009 with a history of hypothermia-treated HIE.
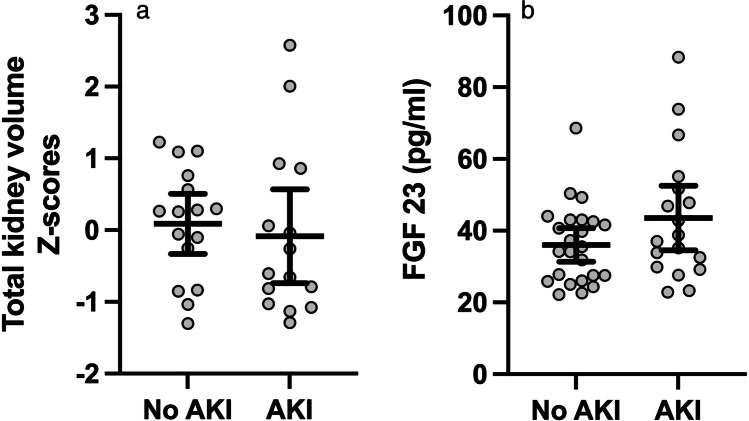
At 10-12 years of age, we measured cystatin C (cyst C) to estimate GFR. Children with decreased cyst C eGFR also underwent iohexol clearance examination. We measured urine-albumin/creatinine ratio, blood pressure (BP) and kidney volume on magnetic resonance imaging. Fibroblast growth factor 23 (FGF 23) levels in plasma were assessed by enzyme-linked immunosorbent assay (ELISA). Outcomes were compared between children with and without a history of neonatal AKI.
Forty-seven children participated in the assessment. Two children (2/42) had decreased cyst C eGFR, for one of whom iohexol clearance confirmed mildly decreased GFR. One child (1/43) had Kidney Disease Improving Global Outcomes (KDIGO) category A2 albuminuria, and three (3/45) had elevated office BP. Subsequent ambulatory 24-h BP measurement confirmed high normal BP in one case only. No child had hypertension. Kidney volume and FGF 23 levels were normal in all children. There was no difference in any of the parameters between children with and without a history of neonatal AKI.
Renal sequelae were rare in early adolescence following hypothermia-treated HIE regardless of presence or absence of neonatal AKI. A higher resolution version of the Graphical abstract is available as Supplementary information.
在接受低温治疗的缺氧缺血性脑病(HIE)的婴儿中,急性肾损伤(AKI)仍然很常见。关于低温治疗后长期肾脏结局的信息知之甚少。我们最近报告称,接受低温治疗的 HIE 幸存者中有 21%在青少年早期根据血浆肌酐估算肾小球滤过率(eGFR)降低。在这里,我们在斯德哥尔摩出生于 2007-2009 年的接受低温治疗的 HIE 患儿的基于人群的队列中更全面地评估了肾脏功能。
在 10-12 岁时,我们测量胱抑素 C(cyst C)以估算 GFR。胱抑素 C eGFR 降低的儿童还接受了 iohexol 清除检查。我们测量了尿液白蛋白/肌酐比、血压(BP)和磁共振成像的肾脏体积。通过酶联免疫吸附试验(ELISA)评估血浆中成纤维细胞生长因子 23(FGF 23)水平。比较了有和无新生儿 AKI 病史的儿童之间的结果。
47 名儿童参与了评估。2 名儿童(2/42)的胱抑素 C eGFR 降低,其中 1 名儿童的 iohexol 清除证实 GFR 轻度降低。1 名儿童(1/43)有肾脏疾病改善全球结局(KDIGO)A2 白蛋白尿,3 名(3/45)的儿童血压升高。随后的动态 24 小时血压测量仅在 1 例中证实血压偏高。没有儿童患有高血压。所有儿童的肾脏体积和 FGF 23 水平均正常。有和无新生儿 AKI 病史的儿童在任何参数上均无差异。
无论是否存在新生儿 AKI,接受低温治疗的 HIE 后,青少年早期肾脏后遗症罕见。更清晰的图表摘要版本可在补充资料中查看。