Department of Health Behavior and Health Systems, School of Public Health, University of North Texas Health Science Center, 3500 Camp Bowie Blvd., Fort Worth, TX, 76107, USA.
Department of Biostatistics and Epidemiology, University of North Texas Health Science Center, Fort Worth, TX, 76107, USA.
Prev Sci. 2023 Nov;24(8):1608-1621. doi: 10.1007/s11121-022-01420-1. Epub 2022 Aug 17.
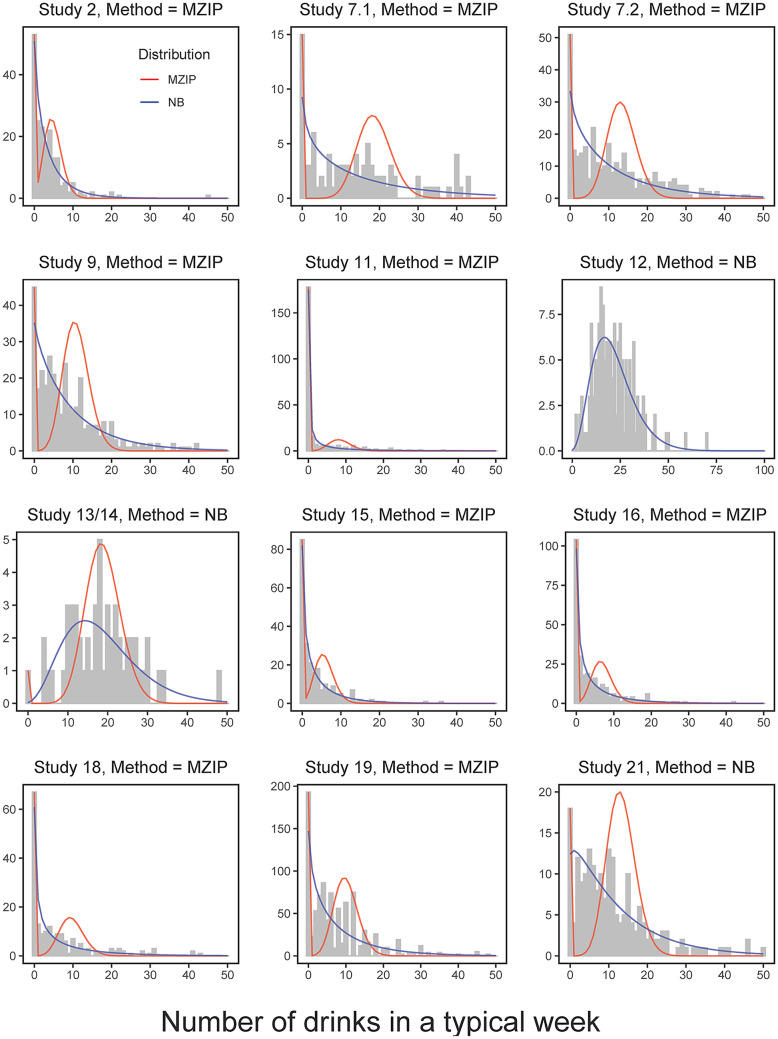
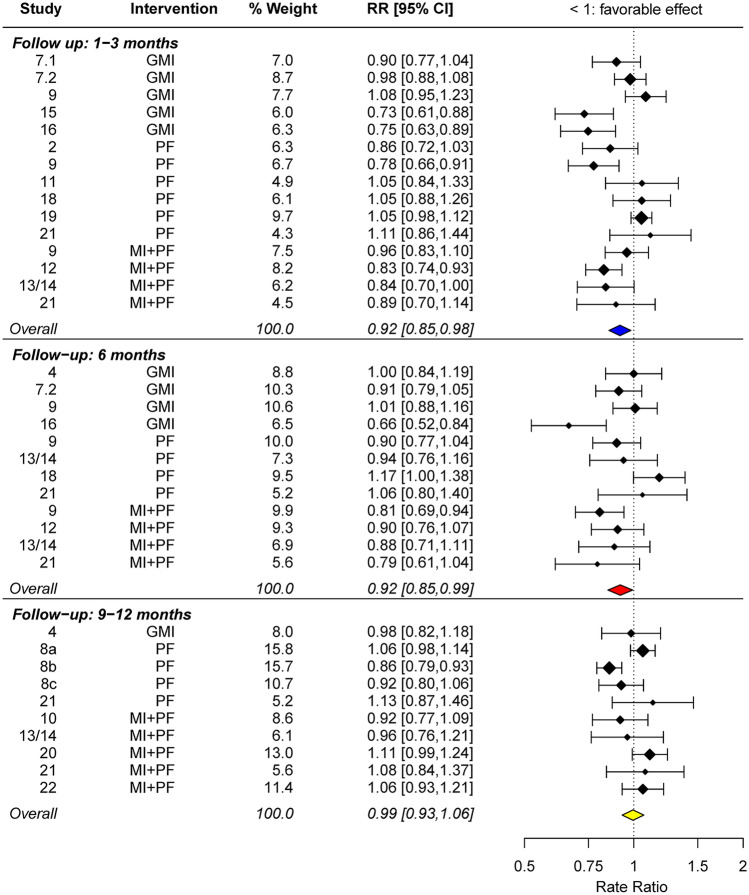
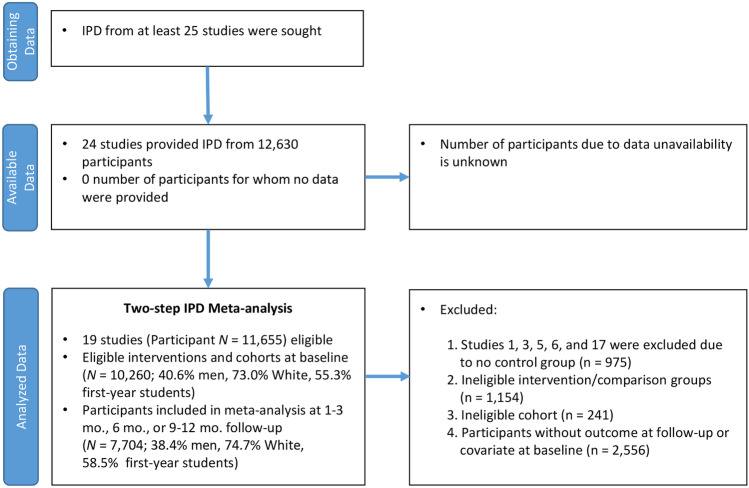
To evaluate and optimize brief alcohol interventions (BAIs), it is critical to have a credible overall effect size estimate as a benchmark. Estimating such an effect size has been challenging because alcohol outcomes often represent responses from a mixture of individuals: those at high risk for alcohol misuse, occasional nondrinkers, and abstainers. Moreover, some BAIs exclusively focus on heavy drinkers, whereas others take a universal prevention approach. Depending on sample characteristics, the outcome distribution might have many zeros or very few zeros and overdispersion; consequently, the most appropriate statistical model may differ across studies. We synthesized individual participant data (IPD) from 19 studies in Project INTEGRATE (Mun et al., 2015b) that randomly allocated participants to intervention and control groups (N = 7,704 participants, 38.4% men, 74.7% White, 58.5% first-year students). We sequentially estimated marginalized zero-inflated Poisson (Long et al., 2014) or negative binomial regression models to obtain covariate-adjusted, study-specific intervention effect estimates in the first step, which were subsequently combined in a random-effects meta-analysis model in the second step. BAIs produced a statistically significant 8% advantage in the mean number of drinks at both 1-3 months (RR = 0.92, 95% CI = [0.85, 0.98]) and 6 months (RR = 0.92, 95% CI = [0.85, 0.99]) compared to controls. At 9-12 months, there was no statistically significant difference in the mean number of drinks between BAIs and controls. In conclusion, BAIs are effective at reducing the mean number of drinks through at least 6 months post intervention. IPD can play a critical role in deriving findings that could not be obtained in original individual studies or standard aggregate data meta-analyses.
为了评估和优化简短的酒精干预措施(BAIs),拥有一个可靠的总体效果大小估计作为基准至关重要。由于酒精的结果通常代表了来自混合人群的反应:那些有酗酒高风险的人、偶尔不饮酒者和戒酒者。此外,一些 BAIs 专门针对重度饮酒者,而另一些则采取普遍预防的方法。根据样本特征,结果分布可能有很多零值或很少的零值和过分散;因此,最合适的统计模型可能因研究而异。我们综合了 Project INTEGRATE(Mun 等人,2015b)中 19 项研究的个体参与者数据(IPD),这些研究随机将参与者分配到干预组和对照组(N = 7704 名参与者,38.4%为男性,74.7%为白人,58.5%为一年级学生)。我们依次估计边缘化零膨胀泊松(Long 等人,2014)或负二项回归模型,以在第一步获得调整协变量的、特定于研究的干预效果估计值,然后在第二步将这些估计值合并到随机效应荟萃分析模型中。与对照组相比,BAIs 在 1-3 个月(RR = 0.92,95%CI = [0.85, 0.98])和 6 个月(RR = 0.92,95%CI = [0.85, 0.99])时,平均饮酒量分别有统计学上的 8%优势。在 9-12 个月时,BAIs 与对照组之间的平均饮酒量没有统计学上的显著差异。总之,BAIs 在至少 6 个月的干预后能够有效地减少平均饮酒量。IPD 可以在原始个体研究或标准汇总数据荟萃分析中发挥关键作用,得出无法获得的发现。