Department of Oncology, University of Calgary, Calgary, Alberta, Canada.
Department of Public Health Sciences, University of Alberta, Edmonton, Alberta, Canada.
JAMA Netw Open. 2022 Aug 1;5(8):e2227225. doi: 10.1001/jamanetworkopen.2022.27225.
Risk prediction models are important to identify survivors of childhood cancer who are at risk of experiencing poor health-related quality of life (HRQOL) as they age.
To develop and validate prediction models for a decline in HRQOL among adult survivors of childhood cancer.
DESIGNS, SETTING, AND PARTICIPANTS: This prognostic study included 4755 adults from the Childhood Cancer Survivor Study (CCSS) diagnosed between January 5, 1970, and December 31, 1986, who completed baseline (time 0 [November 3, 1992, to August 28, 2003]) and 2 follow-up (time 1 [February 12, 2002, to May 21, 2005] and time 2 [January 6, 2014, to November 30, 2016]) surveys. Data were analyzed from June 19, 2019, to February 2, 2022.
Sociodemographic, lifestyle, and emotional factors, and chronic health conditions (CHCs) were assessed at time 0 and time 1, and neurocognitive factors were assessed at time 1 to predict HRQOL at time 2 and a decline in HRQOL between time 1 and time 2. Impaired health states were defined as CHC grades 2 to 4 using the modified Common Terminology Criteria for Adverse Events, version 4.03, and mental and neurocognitive status as 1 SD or more below reference levels.
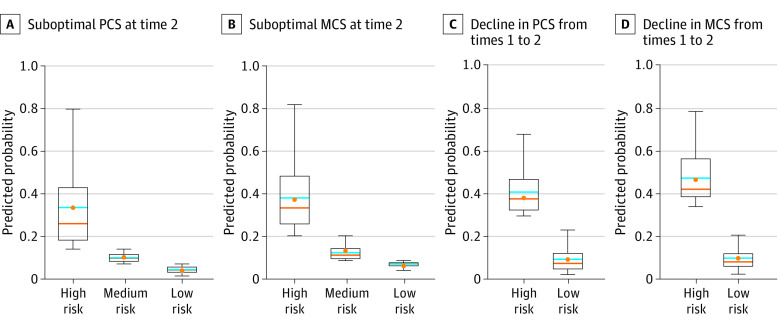
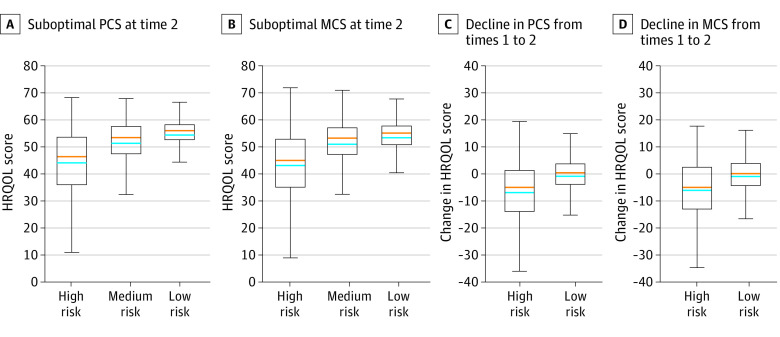
Health-related quality of life was operationalized using the Medical Outcomes Study 36-Item Short Form Health Survey Physical (PCS) and Mental (MCS) Component Summary and classified by optimal (≥40) or suboptimal (<40) at each point (main outcome). A decline in HRQOL was defined as a change from optimal to suboptimal between time 1 and time 2. Multivariable logistic regression identified factors associated with HRQOL decline. The cohort was randomly split into training (80%) and test (20%) data sets for model development and validation; the area under the receiver operating characteristic curve was used to evaluate prediction performance.
A total of 4755 adults (mean [SD] age at time 0, 24.3 [7.6] years; 2623 [55.2%] women) were included in the analysis. Between time 1 and time 2, 285 of 3294 survivors (8.7%) had declining PCS and 278 of 3294 (8.4%) had declining MCS. Risk factors associated with PCS decline included female sex (odds ratio [OR], 1.67 [95% CI, 1.25-2.24]), family income less than $20 000 vs $80 000 or more (OR, 2.00 [95% CI, 1.21-3.30]), presence of CHCs (OR for neurological, 2.16 [95% CI, 1.51-3.10]; OR for endocrine, 2.25 [95% CI, 1.44-3.52]; OR for gastrointestinal tract, 1.89 [95% CI, 1.32-2.69]; OR for respiratory, 1.66 [95% CI, 1.06-2.59]; OR for cardiovascular, 1.53 [95% CI, 1.14-2.06]), and depression (OR, 1.79 [95% CI, 1.20-2.67]). Risk factors associated with MCS decline included unemployment vs full-time employment (OR, 1.68; [95% CI, 1.19-2.38]), current vs never cigarette smoking (OR, 2.03 [95% CI, 1.37-3.00]), depression (OR, 4.29 [95% CI, 2.44-7.55]), somatization (OR, 1.63 [95% CI, 1.05-2.53]), impaired task efficiency (OR, 1.90 [95% CI, 1.34-2.68]), and impaired organization (OR, 1.67 [95% CI, 1.12-2.48]). The areas under the receiver operating characteristic curve for the test models were 0.74 (95% CI, 0.67-0.81) for declining PCS and 0.68 (95% CI, 0.60-0.75) for declining MCS.
In this prognostic study of adult survivors of childhood cancer who experienced declining HRQOL, CHCs were associated with a decline in physical HRQOL, whereas current smoking and emotional and neurocognitive impairment were associated with a decline in mental HRQOL. These findings suggest that interventions targeting modifiable risk factors are needed to prevent poor HRQOL in this population.
风险预测模型对于识别儿童癌症幸存者中随着年龄增长健康相关生活质量(HRQOL)下降风险高的幸存者非常重要。
开发和验证儿童癌症幸存者成年后 HRQOL 下降的预测模型。
设计、地点和参与者:本预后研究纳入了来自儿童癌症幸存者研究(CCSS)的 4755 名成年人,他们于 1970 年 1 月 5 日至 1986 年 12 月 31 日被诊断为儿童癌症,完成了基线(时间 0 [1992 年 11 月 3 日至 2003 年 8 月 28 日])和 2 次随访(时间 1 [2002 年 2 月 12 日至 2005 年 5 月 21 日]和时间 2 [2014 年 1 月 6 日至 2016 年 11 月 30 日])调查。数据分析于 2019 年 6 月 19 日至 2022 年 2 月 2 日进行。
在时间 0 和时间 1 评估社会人口统计学、生活方式和情绪因素以及慢性健康状况(CHC),并在时间 1 评估神经认知因素,以预测时间 2 的 HRQOL 和时间 1 与时间 2 之间的 HRQOL 下降。使用改良的常见不良事件术语标准 4.03,将 CHC 等级 2 至 4 定义为受损健康状态,将精神和神经认知状态定义为低于参考水平 1 个标准差或更低。
使用医疗结局研究 36 项简短健康调查物理(PCS)和心理(MCS)分量总结来操作化健康相关生活质量,并在每个时间点(主要结果)将其分为最佳(≥40)或次优(<40)。HRQOL 下降定义为时间 1 与时间 2 之间从最佳到次优的变化。多变量逻辑回归确定了与 HRQOL 下降相关的因素。该队列被随机分为训练(80%)和测试(20%)数据集进行模型开发和验证;接受者操作特征曲线下面积用于评估预测性能。
共有 4755 名成年人(时间 0 时的平均[SD]年龄,24.3[7.6]岁;女性 2623 人[55.2%])纳入分析。在时间 1 和时间 2 之间,3294 名幸存者中的 285 名(8.7%)PCS 下降,3294 名幸存者中的 278 名(8.4%)MCS 下降。与 PCS 下降相关的危险因素包括女性(优势比[OR],1.67[95%置信区间,1.25-2.24])、家庭收入低于 20000 美元与 80000 美元或以上(OR,2.00[95%置信区间,1.21-3.30])、存在 CHC(OR 神经科,2.16[95%置信区间,1.51-3.10];OR 内分泌科,2.25[95%置信区间,1.44-3.52];OR 胃肠道科,1.89[95%置信区间,1.32-2.69];OR 呼吸科,1.66[95%置信区间,1.06-2.59];OR 心血管科,1.53[95%置信区间,1.14-2.06])和抑郁(OR,1.79[95%置信区间,1.20-2.67])。与 MCS 下降相关的危险因素包括失业与全职就业(OR,1.68[95%置信区间,1.19-2.38])、当前吸烟与从不吸烟(OR,2.03[95%置信区间,1.37-3.00])、抑郁(OR,4.29[95%置信区间,2.44-7.55])、躯体化(OR,1.63[95%置信区间,1.05-2.53])、任务效率受损(OR,1.90[95%置信区间,1.34-2.68])和组织受损(OR,1.67[95%置信区间,1.12-2.48])。测试模型的接收者操作特征曲线下面积为 0.74(95%置信区间,0.67-0.81),用于下降 PCS,0.68(95%置信区间,0.60-0.75),用于下降 MCS。
在这项对经历 HRQOL 下降的成年儿童癌症幸存者的预后研究中,CHC 与身体 HRQOL 下降相关,而当前吸烟和情绪和神经认知障碍与心理 HRQOL 下降相关。这些发现表明,需要针对可改变的风险因素进行干预,以预防该人群的不良 HRQOL。