Department of Biostatistics, Vanderbilt University Medical Center, Nashville, Tennessee.
Center for Quantitative Sciences, Vanderbilt University Medical Center, Nashville, Tennessee.
JAMA Netw Open. 2022 Aug 1;5(8):e2227211. doi: 10.1001/jamanetworkopen.2022.27211.
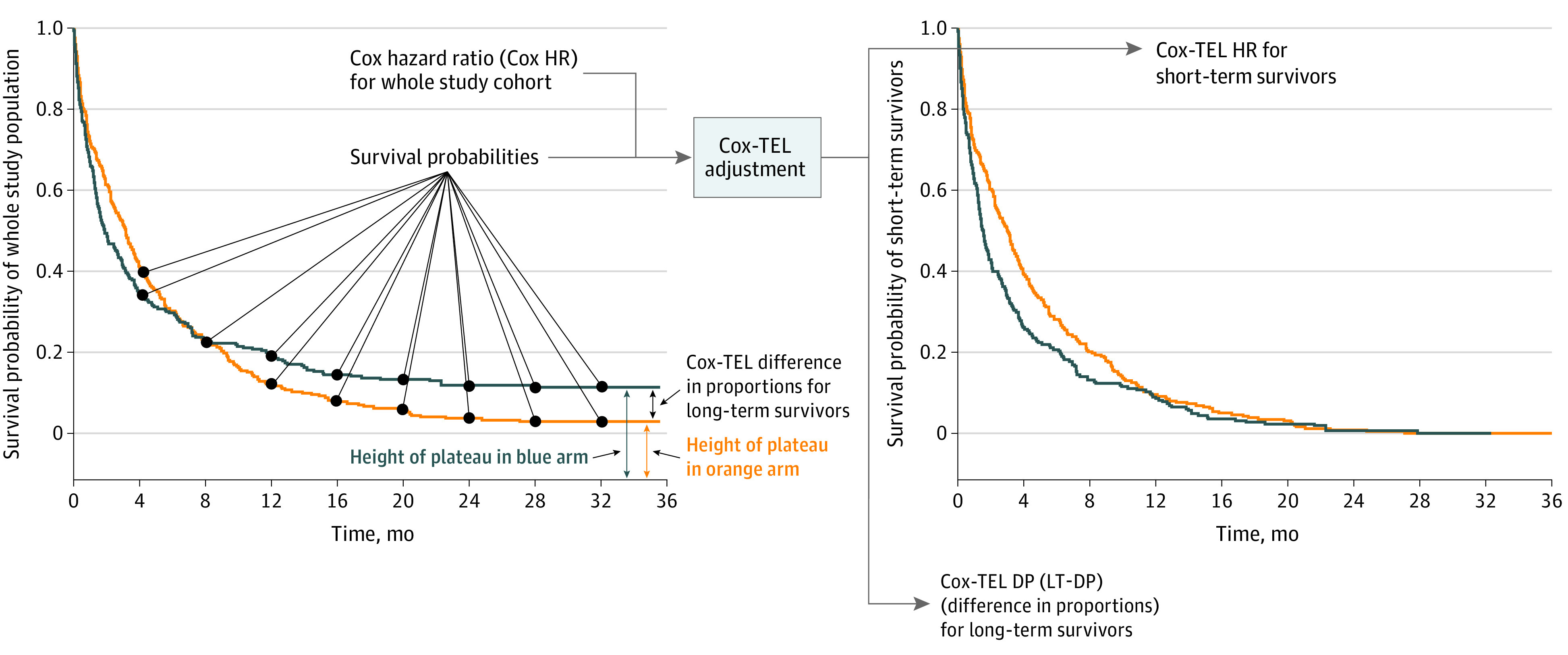
Appropriate clinical decision-making relies on accurate data interpretation, which in turn relies on the use of suitable statistical models. Long tails and early crossover-2 features commonly observed in immune checkpoint inhibitor (ICI) survival curves-raise questions as to the suitability of Cox proportional hazards regression for ICI survival analysis. Cox proportional hazards-Taylor expansion adjustment for long-term survival data (Cox-TEL) adjustment may provide possible solutions in this setting.
To estimate overall survival and progression-free survival benefits of ICI therapy vs chemotherapy using Cox-TEL adjustment.
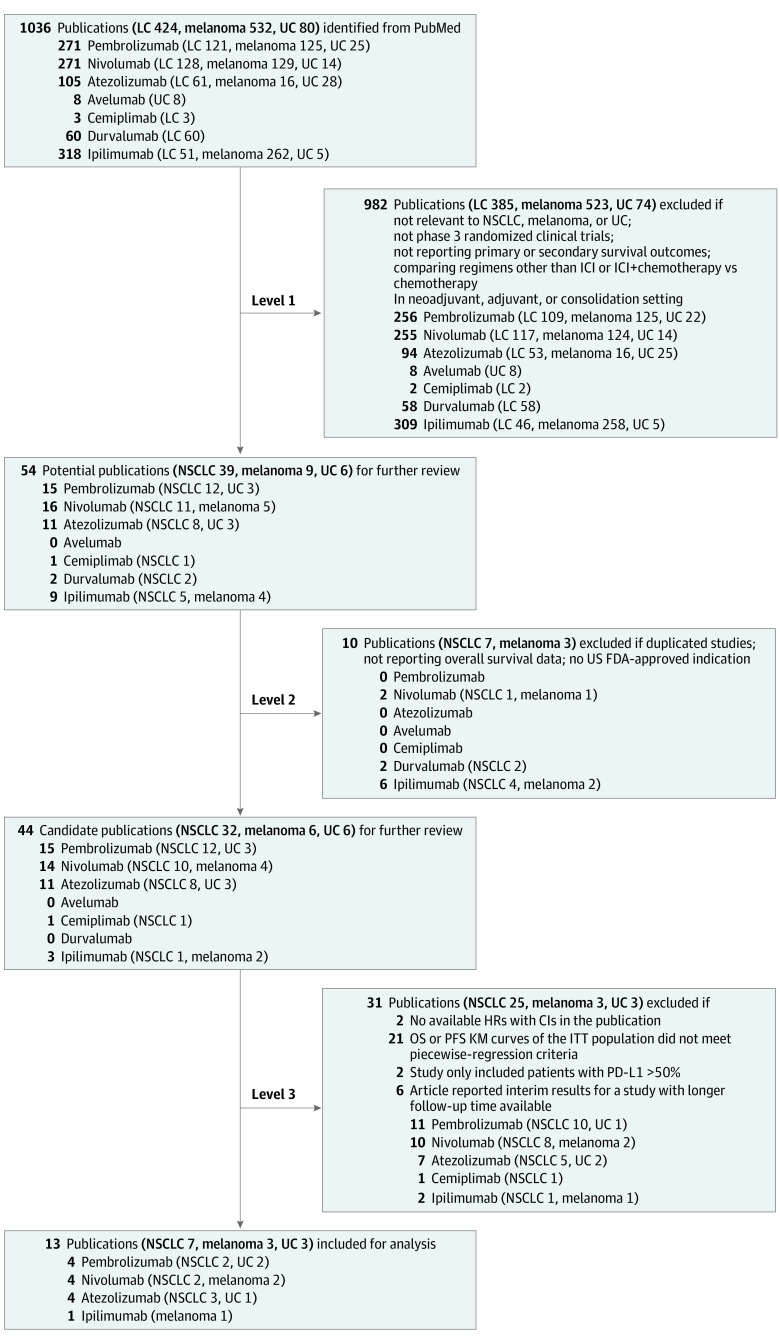
A PubMed search was performed for all cataloged publications through May 22, 2022.
The search was restricted to randomized clinical trials with search terms for ICIs and lung cancer, melanoma, or urothelial carcinoma. The publications identified were further reviewed for inclusion.
Cox proportional hazards ratios (HRs) were transformed to Cox-TEL HRs for patients with short-term treatment response (ie, short-term survivor) (ST-HR) and difference in proportions for patients with long-term survival (LT-DP) by Cox-TEL. Meta-analyses were performed using a frequentist random-effects model.
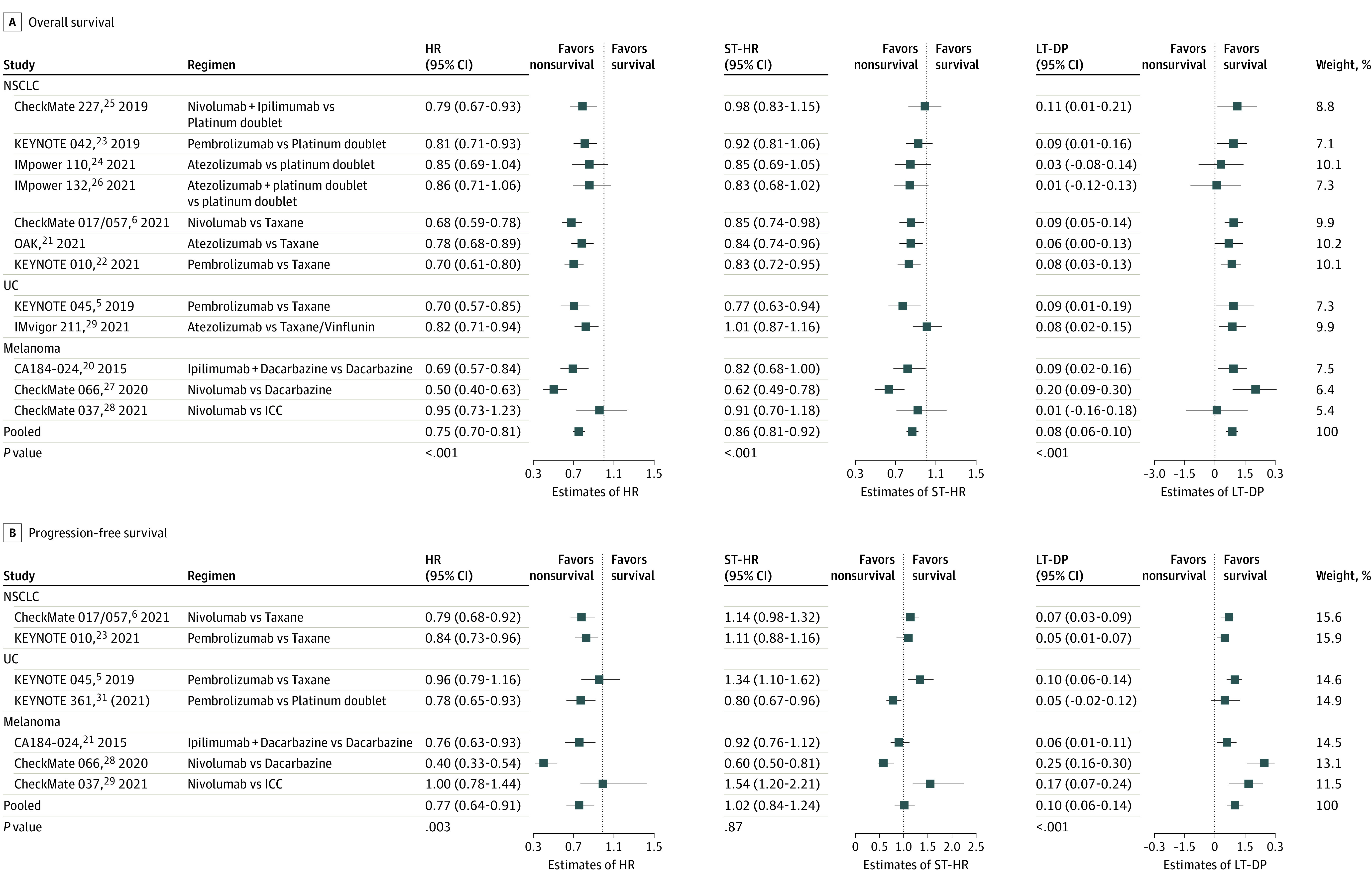
Outcomes of interest were pooled overall survival (primary outcome) and progression-free survival (secondary outcome) HRs, ST-HRs, and LT-DPs. Subgroup analyses stratified by cancer type also were performed.
A total of 1036 publications was identified. After 3 levels of review against inclusion criteria, 13 clinical trials (7 in non-small cell lung cancer, 3 in melanoma, and 3 in urothelial carcinoma) were selected for the meta-analysis. In the primary analysis, pooled findings were 0.75 (95% CI, 0.70-0.81) for HR, 0.86 (95% CI, 0.81-0.92) for ST-HR, and 0.08 (95% CI, 0.06-0.10) for LT-DP. In the secondary analysis, the pooled values for progression-free survival were 0.77 (95% CI, 0.64-0.91) for HR, 1.02 (95% CI, 0.84-1.24) for ST-HR, and 0.10 (95% CI, 0.06-0.14) for LT-DP.
This systematic review and meta-analysis of ICI clinical trial results noted consistently larger ST-HRs vs Cox HRs for ICI therapy, with an LT-DP of approximately 10%. These results suggest that Cox HRs may not provide a full picture of survival outcomes when the risk reduction from treatment is not constant, which may aid in the decision-making process of oncologists and patients.
准确的数据解释依赖于恰当的临床决策,而这又依赖于合适的统计模型的使用。免疫检查点抑制剂(ICI)生存曲线中常见的长尾和早期交叉-2 特征引发了关于 Cox 比例风险回归是否适合 ICI 生存分析的问题。Cox 比例风险-用于长期生存数据的泰勒扩展调整(Cox-TEL)调整可能在这种情况下提供可能的解决方案。
使用 Cox-TEL 调整估计 ICI 治疗与化疗相比的总生存和无进展生存获益。
通过 2022 年 5 月 22 日的 PubMed 搜索,对所有编目出版物进行了搜索。
搜索仅限于随机临床试验,使用 ICI 和肺癌、黑色素瘤或尿路上皮癌的搜索词。进一步审查确定的出版物以纳入。
通过 Cox-TEL 将 Cox 比例风险比(HR)转换为短期治疗反应(即短期幸存者)(ST-HR)的 Cox-TEL HR 和长期幸存者(LT-DP)的比例差异。使用频率论随机效应模型进行荟萃分析。
感兴趣的结果是汇总总生存(主要结果)和无进展生存(次要结果)HR、ST-HR 和 LT-DP。还按癌症类型进行了亚组分析。
共确定了 1036 篇出版物。经过 3 级纳入标准审查,选择了 13 项临床试验(7 项非小细胞肺癌、3 项黑色素瘤和 3 项尿路上皮癌)进行荟萃分析。在主要分析中,HR 的合并发现为 0.75(95%CI,0.70-0.81),ST-HR 为 0.86(95%CI,0.81-0.92),LT-DP 为 0.08(95%CI,0.06-0.10)。在次要分析中,无进展生存的合并值为 HR 为 0.77(95%CI,0.64-0.91),ST-HR 为 1.02(95%CI,0.84-1.24),LT-DP 为 0.10(95%CI,0.06-0.14)。
本系统评价和 ICI 临床试验结果的荟萃分析指出,ICI 治疗的 ST-HR 始终明显大于 Cox HR,LT-DP 约为 10%。这些结果表明,当治疗的风险降低不是恒定时,Cox HR 可能无法全面反映生存结果,这可能有助于肿瘤学家和患者的决策过程。