Vanderbilt Center for Child Health Policy, Vanderbilt University Medical Center, Nashville, Tennessee.
Department of Pediatrics, Vanderbilt University Medical Center, Nashville, Tennessee.
JAMA Health Forum. 2021 Oct 29;2(10):e213470. doi: 10.1001/jamahealthforum.2021.3470. eCollection 2021 Oct.
The opioid crisis has increasingly affected pregnant people and infants. Hepatitis C virus (HCV) infections, a known complication of opioid use, grew in parallel with opioid-related complications; however, the literature informing individual and community risks associated with maternal HCV infection is sparse.
To determine (1) individual and county-level factors associated with HCV among pregnant people and their newborn infants, and (2) how county-level factors influence individual risk among the highest risk individuals.
This time-series analysis of retrospective, repeated cross-sectional data included pregnant people in all US counties from 2009 to 2019. We constructed mixed-effects logistic regression models to explore the association between HCV infection and individual and county-level covariates. Analyses were conducted between June 2019 and September 2021.
Individual-level: race and ethnicity, education, marital status, insurance type; county-level: rurality, employment, density of obstetricians.
Hepatitis C virus as indicated on the newborn's birth certificate.
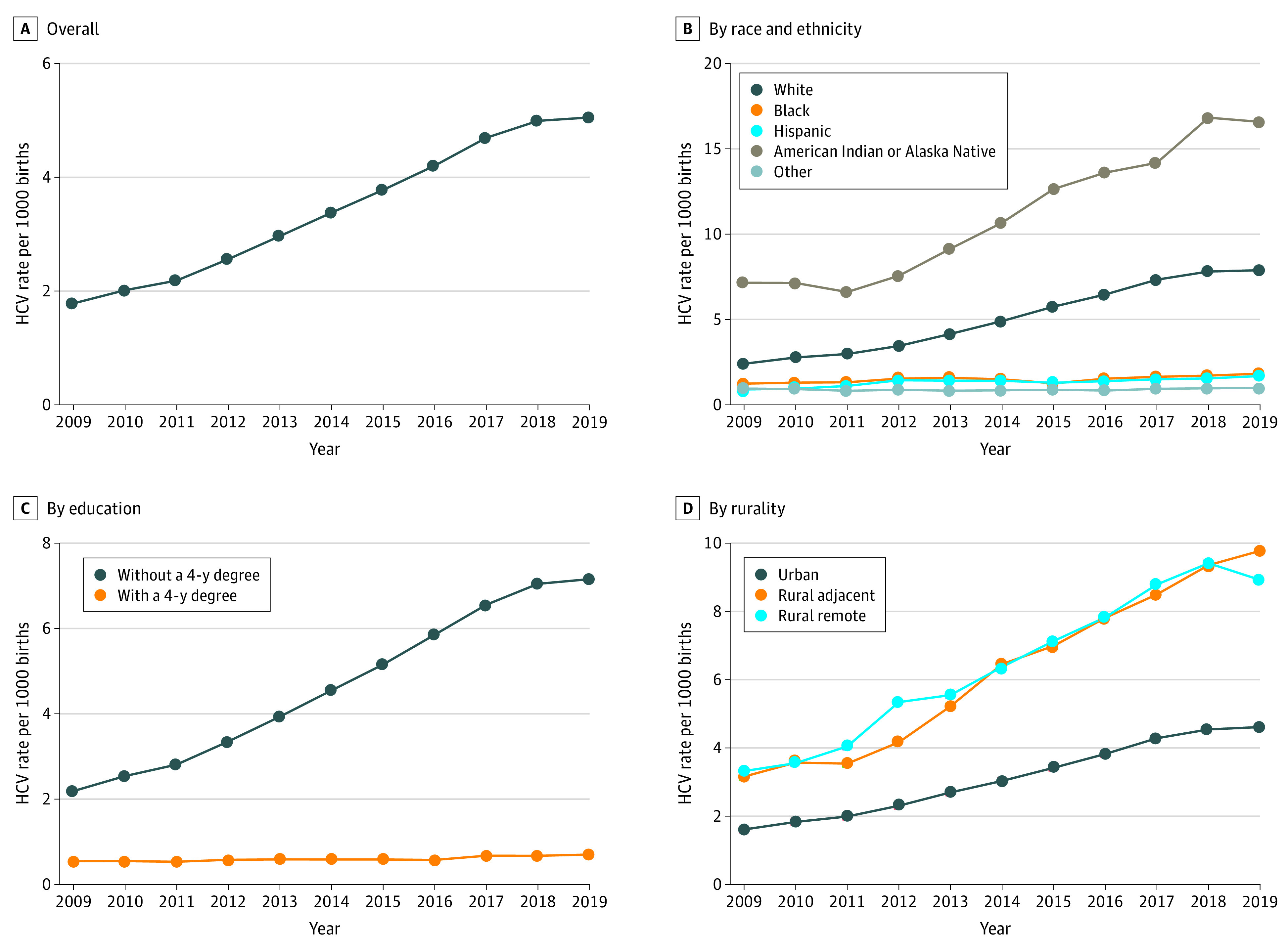
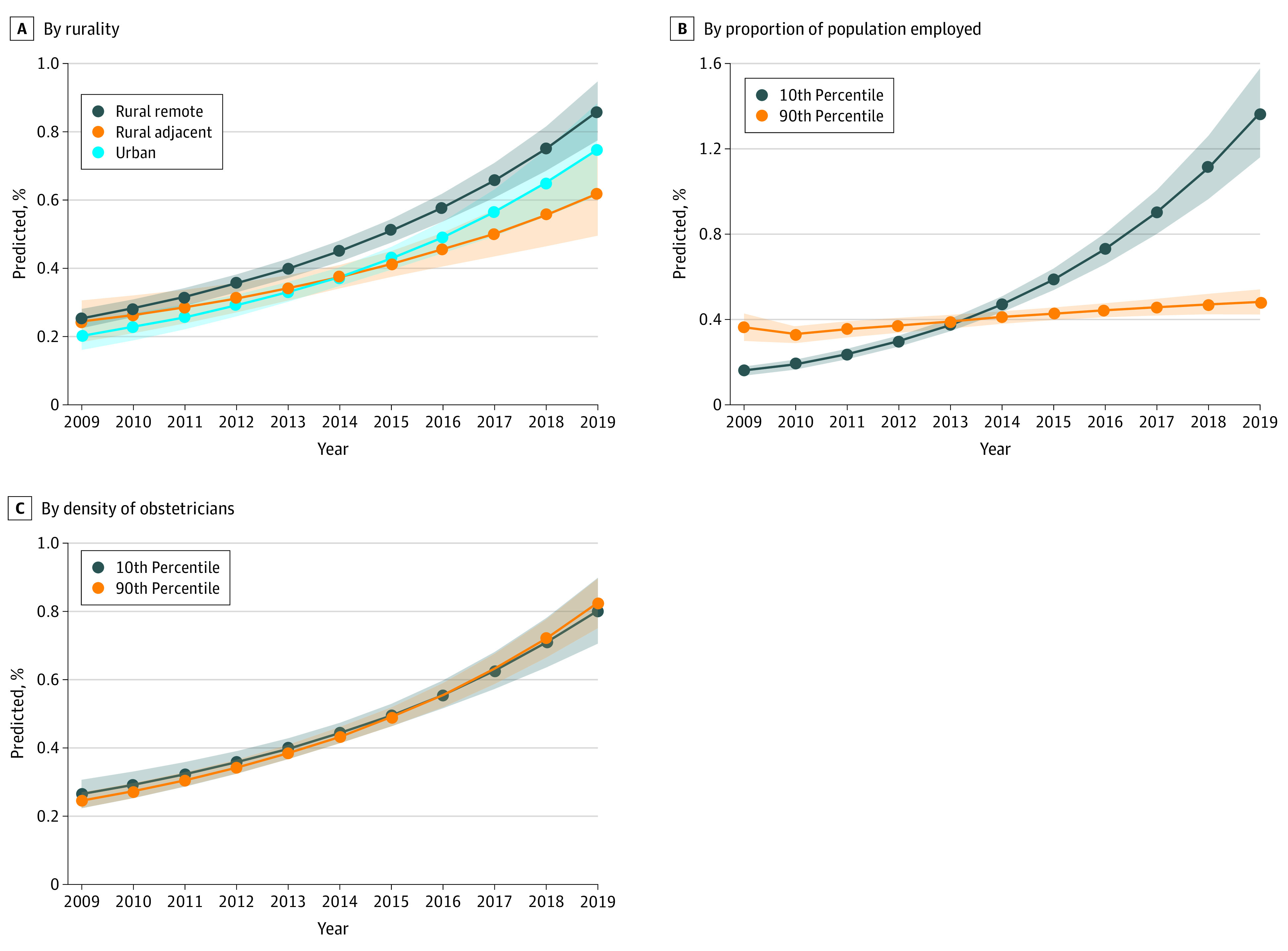
Between 2009 and 2019, there were 39 380 122 pregnant people who met inclusion criteria, among whom 138 343 (0.4%) were diagnosed with HCV. People with HCV were more likely to be White (79.9% vs 53.5%), American Indian or Alaska Native (AI/AN) (2.9% vs 0.9%), be without a 4-year degree (93.2% vs 68.6%), and be unmarried (73.7% vs 38.8%). The rate (per 1000 live births) of HCV among pregnant people increased from 1.8 to 5.1. In adjusted analyses, the following factors were associated with higher rates of HCV: individuals identified as White (adjusted odds ratio [aOR], 7.37; 95% CI, 7.20-7.55) and AI/AN (aOR, 7.94; 95% CI, 7.58-8.31) compared with Black individuals, those without a 4-year degree (aOR, 3.19; 95% CI, 3.11-3.28), those with Medicaid vs private insurance (aOR, 3.27; 95% CI, 3.21-3.33), and those who were unmarried (aOR, 2.80; 95% CI, 2.76-2.84); whereas, rural residence, higher rates of employment, and greater density of obstetricians was associated with lower risk of HCV. Among individuals at the highest risk of HCV, higher levels of county employment, accounting for other factors, were associated with less of a rise in HCV infections over time.
In this cross-sectional study, maternal and newborn HCV infections increased substantially between 2009 and 2019, disproportionately among White and AI/AN people without a 4-year degree. County-level factors, including higher levels of employment, were associated with lower individual risks of acquiring the virus.
阿片类药物危机越来越影响到孕妇和婴儿。丙型肝炎病毒(HCV)感染是阿片类药物使用的已知并发症,与阿片类药物相关的并发症同时增加;然而,有关母婴 HCV 感染相关个体和社区风险的文献很少。
确定(1)与孕妇及其新生儿 HCV 相关的个体和县级因素,以及(2)县级因素如何影响最高风险个体的个体风险。
设计、设置和参与者:这是一项回顾性、重复横断面数据分析,包括 2009 年至 2019 年期间美国所有县的孕妇。我们构建了混合效应逻辑回归模型,以探讨 HCV 感染与个体和县级协变量之间的关联。分析于 2019 年 6 月至 2021 年 9 月进行。
个体水平:种族和民族、教育、婚姻状况、保险类型;县级:农村、就业、妇产科医生密度。
新生儿出生证明上的丙型肝炎病毒。
2009 年至 2019 年间,共有 39380122 名符合纳入标准的孕妇,其中 138343 人(0.4%)被诊断为 HCV。患有 HCV 的人更有可能是白人(79.9%比 53.5%)、美国印第安人或阿拉斯加原住民(AI/AN)(2.9%比 0.9%)、没有四年制学位(93.2%比 68.6%)和未婚(73.7%比 38.8%)。孕妇 HCV 的发病率(每 1000 例活产)从 1.8 上升到 5.1。在调整分析中,以下因素与 HCV 发病率较高相关:与黑人个体相比,被认定为白人(调整后的优势比[aOR],7.37;95%CI,7.20-7.55)和 AI/AN(aOR,7.94;95%CI,7.58-8.31)、没有四年制学位(aOR,3.19;95%CI,3.11-3.28)、拥有医疗补助而不是私人保险(aOR,3.27;95%CI,3.21-3.33)和未婚(aOR,2.80;95%CI,2.76-2.84);而农村居住、较高的就业率和较高的妇产科医生密度与较低的 HCV 风险相关。在 HCV 风险最高的个体中,较高的县就业水平,在考虑到其他因素的情况下,与 HCV 感染随时间的上升幅度较小有关。
在这项横断面研究中,2009 年至 2019 年间,母婴 HCV 感染大幅增加,在没有四年制学位的白人、AI/AN 中比例不成比例。县级因素,包括较高的就业率,与个体获得病毒的风险较低有关。