Vanderbilt Center for Child Health Policy, Vanderbilt University Medical Center, Nashville, Tennessee.
Department of Pediatrics, Vanderbilt University Medical Center, Nashville, Tennessee.
JAMA Netw Open. 2020 Aug 3;3(8):e2013456. doi: 10.1001/jamanetworkopen.2020.13456.
Medications for opioid use disorder, including buprenorphine hydrochloride and methadone hydrochloride, are highly effective at improving outcomes for individuals with the disorder. For pregnant women, use of these medications also improves pregnancy outcomes, including the risk of preterm birth. Despite the known benefits of medications for opioid use disorder, many pregnant and nonpregnant women with the disorder are not receiving them.
To determine whether pregnancy and insurance status are associated with a woman's ability to obtain an appointment with an opioid use disorder treatment clinician.
DESIGN, SETTING, AND PARTICIPANTS: In this cross-sectional study with random assignment of clinicians and simulated-patient callers (performed in "secret shopper" format), outpatient clinics that provide buprenorphine and methadone were randomly selected from publicly available treatment lists in 10 US states (selected for variability in opioid-related outcomes and policies) from March 7 to September 5, 2019. Pregnant vs nonpregnant woman and private vs public insurance assigned randomly to callers to create unique patient profiles. Simulated patients called the clinics posing as pregnant or nonpregnant women to obtain an initial appointment with a clinician.
Appointment scheduling, wait time, and out-of-pocket costs.
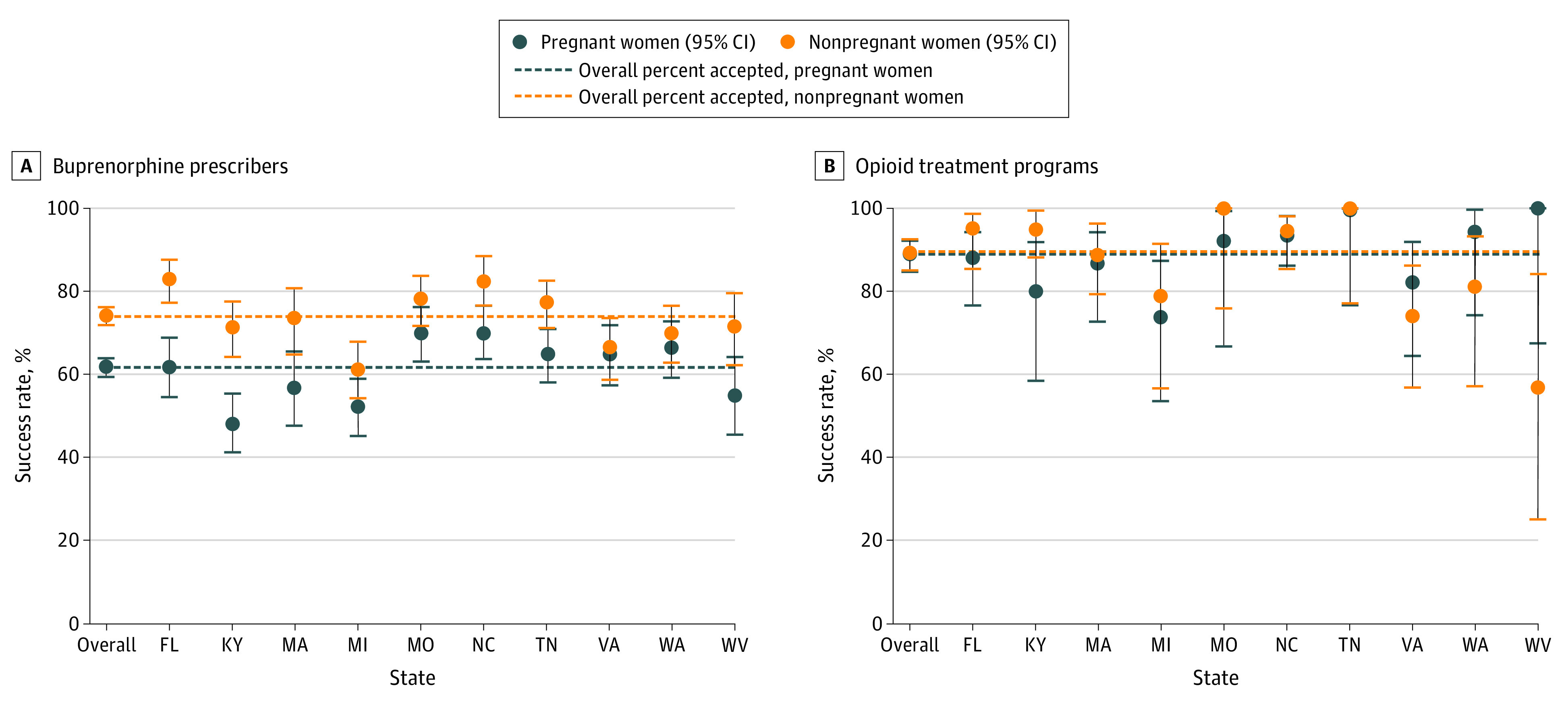
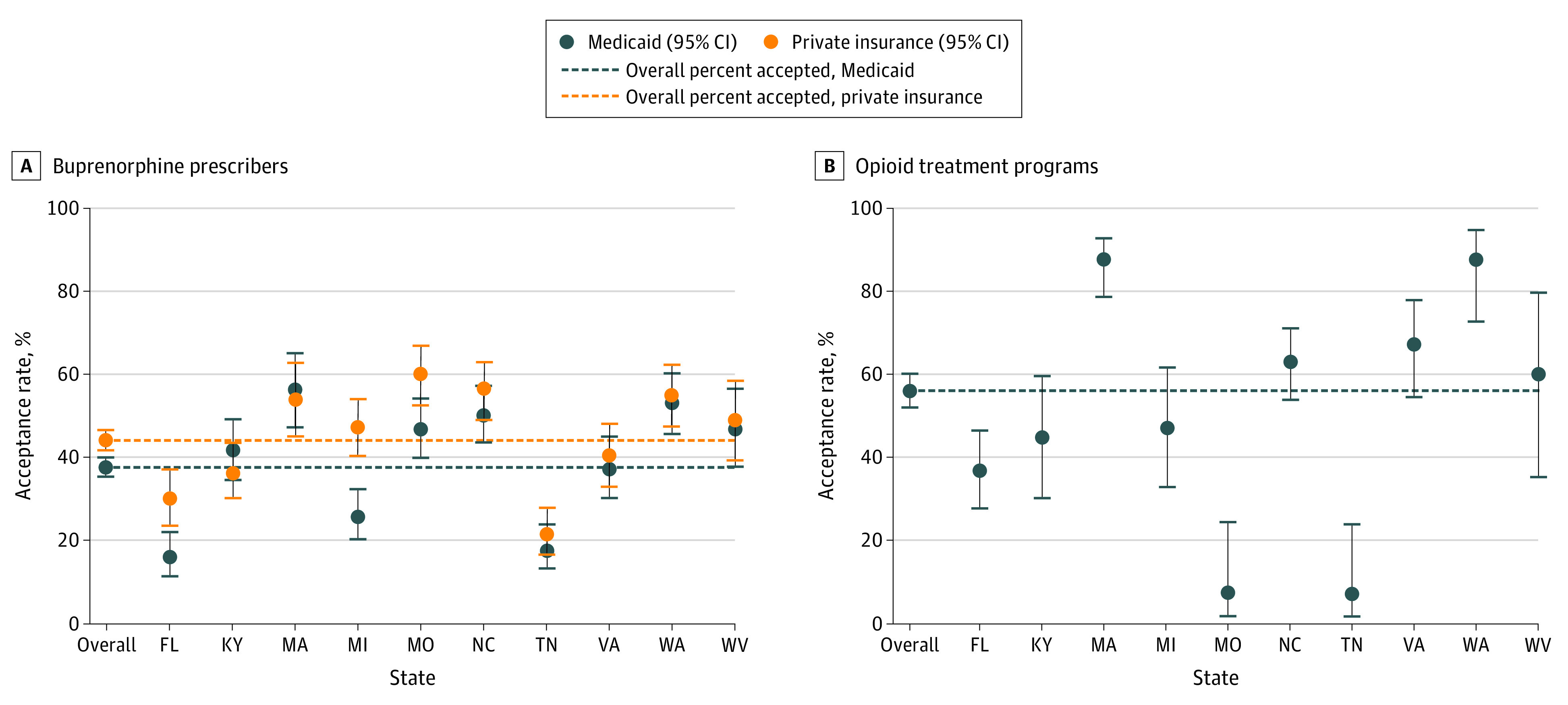
A total of 10 871 unique patient profiles were assigned to 6324 clinicians. Among all women, 2312 of 3420 (67.6%) received an appointment with a clinician who prescribed buprenorphine, with lower rates among pregnant vs nonpregnant callers (1055 of 1718 [61.4%] vs 1257 of 1702 [73.9%]; relative risk, 0.83; 95% CI, 0.79-0.87). For clinicians who prescribed methadone, there was no difference in appointment access for pregnant vs nonpregnant callers (240 of 271 [88.6%] vs 237 of 265 [89.4%]; relative risk, 0.99; 95% CI, 0.93-1.05). Insurance was frequently not accepted, with 894 of 3420 buprenorphine-waivered prescribers (26.1%) and 174 of 536 opioid treatment programs (32.5%) granting appointments only when patients agreed to pay cash. Median wait times did not differ between pregnant and nonpregnant callers among buprenorphine prescribers (3 days [interquartile range, 1-7 days] vs 3 days [interquartile range, 1-7 days]; P = .43) but did differ among methadone prescribers (1 day [interquartile range, 1-4 days] vs 2 days [interquartile range, 1-6 days]; P = .049). For patients agreeing to pay cash, the median out-of-pocket costs for initial appointments were $250 (interquartile range, $155-$300) at buprenorphine prescribers and $34 (interquartile range, $15-$120) at methadone prescribers.
In this cross-sectional study with random assignment of clinicians and simulated-patient callers, many women, especially pregnant women, faced barriers to accessing treatment. Given the high out-of-pocket costs and lack of acceptance of insurance among many clinicians, access to affordable opioid use disorder treatment is a significant concern.
用于治疗阿片类药物使用障碍的药物,包括丁丙诺啡盐酸盐和盐酸美沙酮,在改善该疾病患者的预后方面非常有效。对于孕妇而言,使用这些药物也可以改善妊娠结局,包括早产风险。尽管阿片类药物使用障碍药物有已知的益处,但许多患有该疾病的孕妇和非孕妇并未使用这些药物。
确定妊娠和保险状况是否与女性获得阿片类药物使用障碍治疗临床医生预约的能力相关。
设计、地点和参与者:在这项具有临床医生和模拟患者呼叫者随机分配的横断面研究(以“秘密购物者”的形式进行)中,从美国 10 个州的公开治疗名单中随机选择提供丁丙诺啡和美沙酮的门诊诊所(因阿片类药物相关结果和政策的差异而选择),时间为 2019 年 3 月 7 日至 9 月 5 日。将孕妇与非孕妇以及私人保险与公共保险随机分配给呼叫者,以创建独特的患者档案。模拟患者以孕妇或非孕妇的身份致电诊所,以获得与临床医生的初次预约。
预约安排、等待时间和自付费用。
共分配了 10871 个独特的患者档案给 6324 名临床医生。在所有女性中,3420 名中有 2312 名(67.6%)获得了丁丙诺啡处方临床医生的预约,而孕妇呼叫者的预约率较低(1718 名中有 1055 名[61.4%],1702 名中有 1257 名[73.9%];相对风险,0.83;95%CI,0.79-0.87)。对于开美沙酮的临床医生,孕妇和非孕妇呼叫者的预约机会没有差异(271 名中有 240 名[88.6%],265 名中有 237 名[89.4%];相对风险,0.99;95%CI,0.93-1.05)。保险经常不被接受,3420 名丁丙诺啡豁免处方医生中有 894 名(26.1%),536 个阿片类药物治疗计划中有 174 名(32.5%)仅在患者同意支付现金时才给予预约。丁丙诺啡处方医生中,孕妇和非孕妇呼叫者的中位等待时间没有差异(3 天[四分位距,1-7 天]与 3 天[四分位距,1-7 天];P=0.43),但美沙酮处方医生的等待时间存在差异(1 天[四分位距,1-4 天]与 2 天[四分位距,1-6 天];P=0.049)。对于同意支付现金的患者,初始预约的自付费用中位数为 250 美元(四分位距,155-300 美元)在丁丙诺啡处方医生处,在美沙酮处方医生处为 34 美元(四分位距,15-120 美元)。
在这项具有临床医生和模拟患者呼叫者随机分配的横断面研究中,许多女性,尤其是孕妇,在获得治疗方面面临障碍。鉴于许多临床医生自付费用高且不接受保险,获得负担得起的阿片类药物使用障碍治疗是一个重大问题。