Icahn School of Medicine at Mount Sinai, New York, New York.
James J. Peters Bronx VA Medical Center, Bronx, New York.
JAMA Health Forum. 2022 Feb 11;3(2):e215104. doi: 10.1001/jamahealthforum.2021.5104. eCollection 2022 Feb.
Use of hospice has been demonstrated to be cost saving to the Medicare program and yet the extent to which hospice saves money across all payers, including whether it shifts costs to families, is unknown.
To estimate the association between hospice use and total health care costs including family out-of-pocket health care spending.
This retrospective cohort study of health care spending in the last 6 months of life used data from the nationally representative Medicare Current Beneficiary Survey (MCBS) between the years 2002 and 2018. Participants were MCBS participants who resided in the community and died between 2002 and 2018.
Covariate balancing propensity scores were used to compare participants who used hospice (n = 2113) and those who did not (n = 3351), stratified by duration of hospice use.
Total health care expenditures were measured across payers (family out-of-pocket, Medicare, Medicare Advantage, Medicaid, private insurance, private health maintenance organizations, Veteran's Administration, and other) and by expenditure type (inpatient care, outpatient care, medical visits, skilled nursing, home health, hospice, durable medical equipment, and prescription drugs).
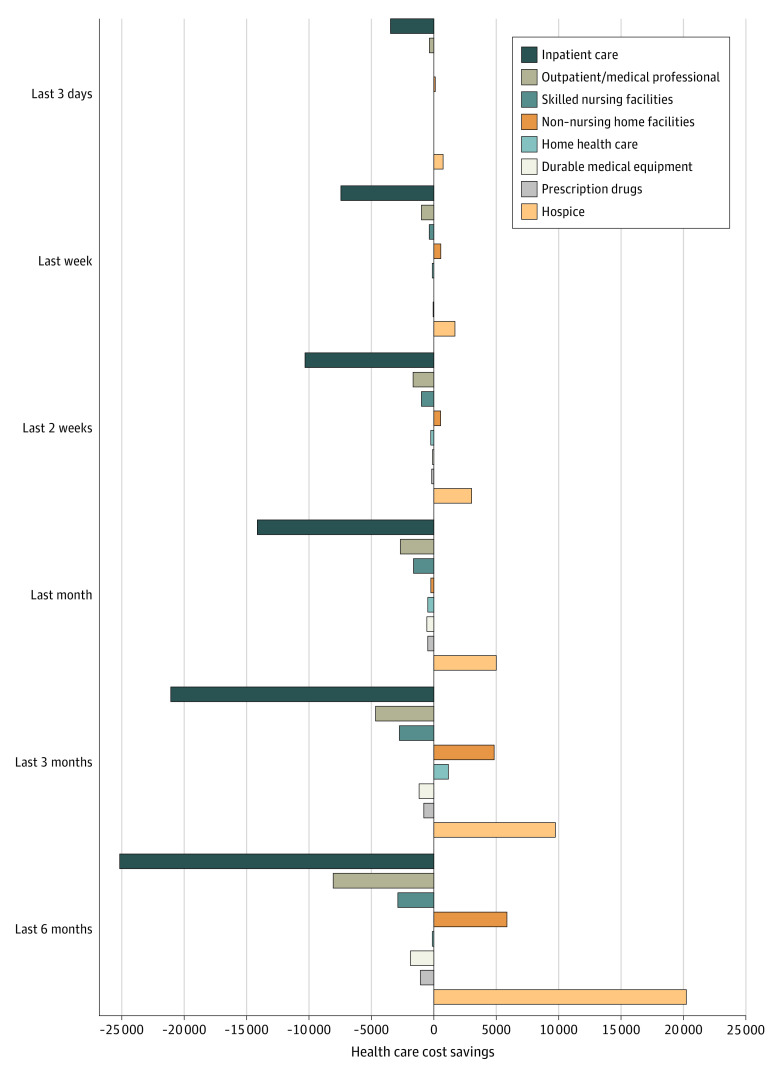
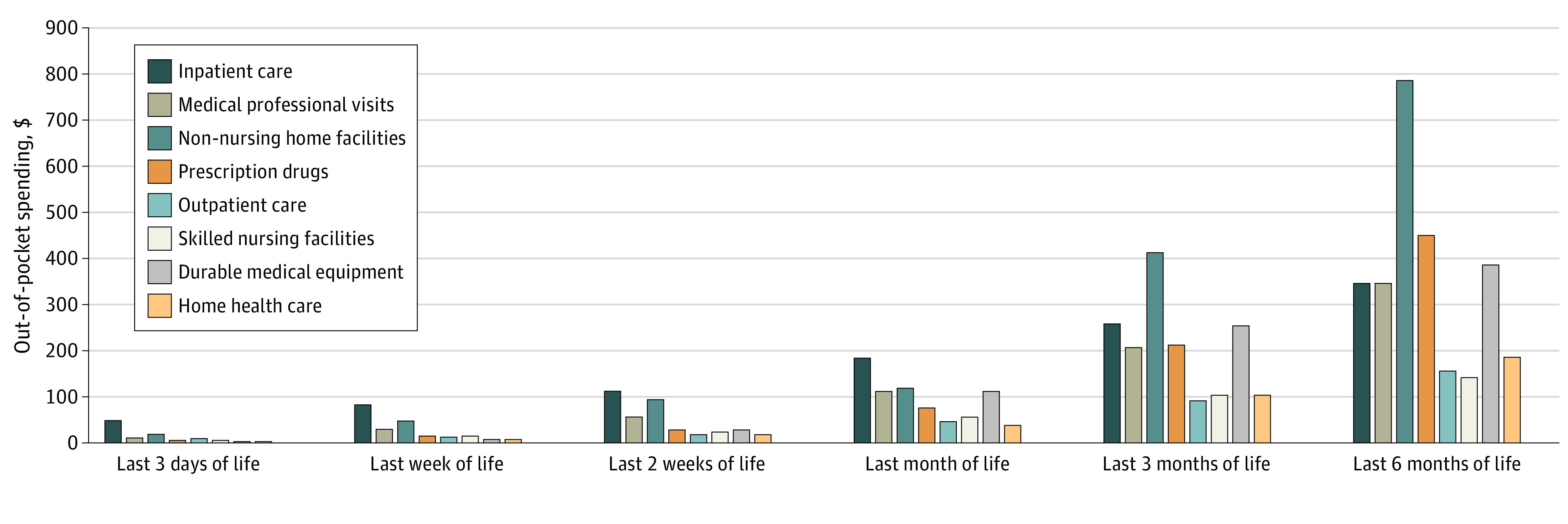
The study population included 5464 decedents (mean age 78.7 years; 48% female) and 38% enrolled with hospice. Total health care expenditures were lower for those who used hospice compared with propensity score weighted non-hospice control participants for the last 3 days of life ($2813 lower; 95% CI, $2396-$3230); last week of life ($6806 lower; 95% CI, $6261-$7350); last 2 weeks of life ($8785 lower; 95% CI, $7971-$9600); last month of life ($11 747 lower; 95% CI, $10 072-$13 422); and last 3 months of life ($10 908 lower; 95% CI, $7283-$14 533). Family out-of-pocket expenditures were lower for hospice enrollees in the last 3 days of life ($71; 95% CI, $43-$100); last week of life ($216; 95% CI, $175-$256); last 2 weeks of life ($265; 95% CI, $149-$382); and last month of life ($670; 95% CI, $530-$811) compared with those who did not use hospice. Health care savings were associated with reductions in inpatient care.
In this population-based cohort study of community-dwelling Medicare beneficiaries, hospice enrollment was associated with lower total health care costs for the last 3 days to 3 months of life. Importantly, we found no evidence of cost shifting from Medicare to families related to hospice enrollment. The magnitude of lower out-of-pocket spending to families who enrolled with hospice is meaningful to many Americans, particularly those with lower socioeconomic status.
已证明使用临终关怀可以为医疗保险计划节省成本,但临终关怀在所有支付方(包括是否将成本转嫁给家庭)节省费用的程度尚不清楚。
评估临终关怀使用与包括家庭自付医疗支出在内的总医疗保健费用之间的关联。
设计、设置和参与者:本研究使用了 2002 年至 2018 年全国代表性医疗保险当前受益人调查(MCBS)的数据,对生命最后 6 个月的医疗保健支出进行了回顾性队列研究。参与者为居住在社区并于 2002 年至 2018 年期间死亡的 MCBS 参与者。
使用协变量平衡倾向评分比较了使用临终关怀(n=2113)和未使用临终关怀(n=3351)的参与者,按临终关怀使用时间长短进行分层。
总医疗保健支出按支付方(家庭自付、医疗保险、医疗保险优势计划、医疗补助、私人保险、私人健康维护组织、退伍军人管理局和其他)和支出类型(住院护理、门诊护理、医疗访视、熟练护理、家庭健康、临终关怀、耐用医疗设备和处方药)进行了衡量。
该研究人群包括 5464 名死者(平均年龄 78.7 岁;48%为女性),其中 38%参加了临终关怀。与经过倾向评分加权的非临终关怀对照组参与者相比,临终关怀组在生命最后 3 天(低 2813 美元;95%CI,2396 美元至 3230 美元)、生命最后 1 周(低 6806 美元;95%CI,6261 美元至 7350 美元)、生命最后 2 周(低 8785 美元;95%CI,7971 美元至 9600 美元)、生命最后 1 个月(低 11747 美元;95%CI,10072 美元至 13422 美元)和生命最后 3 个月(低 10908 美元;95%CI,7283 美元至 14533 美元)的总医疗保健支出较低。临终关怀组在生命最后 3 天(低 71 美元;95%CI,43 美元至 100 美元)、生命最后 1 周(低 216 美元;95%CI,175 美元至 256 美元)、生命最后 2 周(低 265 美元;95%CI,149 美元至 382 美元)和生命最后 1 个月(低 670 美元;95%CI,530 美元至 811 美元)的家庭自付支出也较低。与未使用临终关怀的患者相比,医疗保健储蓄与减少住院护理有关。
在这项基于人群的社区居住的医疗保险受益人的队列研究中,临终关怀登记与生命最后 3 天至 3 个月的总医疗保健费用降低有关。重要的是,我们没有发现临终关怀登记导致医疗保险向家庭转移成本的证据。登记使用临终关怀的家庭自付支出减少的幅度对许多美国人来说意义重大,尤其是那些社会经济地位较低的人。