Duke Margolis Center for Health Policy, Durham, North Carolina.
Department of Pediatrics, Duke University, Durham, North Carolina.
JAMA Health Forum. 2021 Dec 23;2(12):e214283. doi: 10.1001/jamahealthforum.2021.4283. eCollection 2021 Dec.
Brief disruptions in insurance coverage among eligible participants are associated with poorer health outcomes for children.
To describe factors associated with coverage disruptions among children enrolled in North Carolina Medicaid from 2016 to 2018 and estimate the outcome of preventing such disruptions on medical expenditures.
This was a retrospective cohort study using North Carolina Medicaid claims data. All enrolled individuals were aged 1 to 20 years on January 1, 2016, and with 30 days of prior continuous enrollment. Children were observed from January 1, 2016, until December 31, 2018. Analyses were conducted from June 2020 through December 2020.
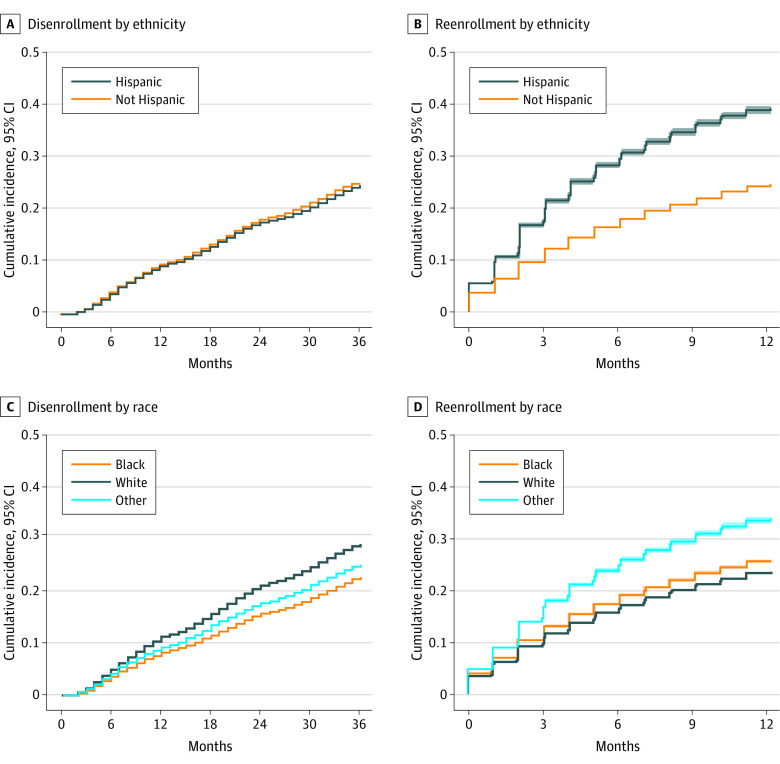
Risk of Medicaid coverage disruptions of 1 to less than 12 months was assessed. Among children who disenrolled from Medicaid for 30 or more days, the risk of reenrollment within 1 to 6 months and 7 to 11 months was assessed. An inverse probability of censoring weights method was then used to estimate the outcome of an intervention to reduce coverage disruptions through preventing disenrollment on per member per month (PMPM) cost.
The study population included 831 173 Medicaid beneficiaries aged 1 to 5 years (23%), 6 to 17 years (68%), and 18 to 20 years (9%); 35% were Black, 44% were White, and 14% were Hispanic/Latinx. Among those with a first disenrollment (n = 214 401, 26%), the risk of reenrollment within 6 months and 7 to 11 months was 19% and 7%, respectively. Risk of coverage disruption was higher for Black children (hazard ratio [HR], 1.21; 95% CI, 1.18-1.24), children of other races (Asian, American Indian, Hawaiian or Pacific Islander, multiple races, or unreported; HR, 1.37; 95% CI, 1.33-1.40), and Latinx children (HR, 1.65; 95% CI, 1.60-1.70) compared with White children. Risk of coverage disruption was also higher for children with higher medical complexity (HR, 1.15; 95% CI, 1.12-1.19). The risk of coverage disruption was lower for children living in counties with the highest unemployment rates (HR, 0.89; 95% CI, 0.85-0.94), and comparisons between county-level measures of child poverty and graduation rates showed little or no difference. The estimated PMPM cost for the full population under a scenario in which all medical costs were included was $125.73. Estimated PMPM cost for the full cohort in a counterfactual scenario in which disenrollment was prevented was slightly lower ($122.14). Across all subgroups, estimated PMPM costs were modestly lower ($2-$8) in the scenario in which disenrollment was prevented.
In this cohort study, the risk of Medicaid coverage disruption was high, with many eligible children in historically marginalized communities continuing to experience unstable enrollment. In addition to improving health outcomes, preventing coverage gaps through policies that decrease disenrollment may also reduce Medicaid costs.
有资格参加的参与者的保险覆盖范围短暂中断与儿童健康结果较差有关。
描述 2016 年至 2018 年北卡罗来纳州医疗补助计划中入组儿童保险覆盖范围中断的相关因素,并估计预防此类中断对医疗支出的影响。
设计、地点和参与者:这是一项回顾性队列研究,使用北卡罗来纳州医疗补助计划的索赔数据。所有入组人员在 2016 年 1 月 1 日年龄为 1 至 20 岁,并且在之前的连续 30 天内有保险。儿童从 2016 年 1 月 1 日观察到 2018 年 12 月 31 日。分析于 2020 年 6 月至 2020 年 12 月进行。
评估 Medicaid 覆盖范围中断的风险为 1 至不到 12 个月。对于 Medicaid 中断 30 天或以上的儿童,评估其在 1 至 6 个月和 7 至 11 个月内重新入组的风险。然后,使用逆概率删失权重法估计通过防止按成员每月(PMPM)成本进行退学来减少覆盖范围中断的干预措施的结果。
研究人群包括 831173 名年龄为 1 至 5 岁(23%)、6 至 17 岁(68%)和 18 至 20 岁(9%)的 Medicaid 受益人;35%为黑人,44%为白人,14%为西班牙裔/拉丁裔。在首次退学的人群中(n=214401,26%),6 个月内和 7 至 11 个月内重新入组的风险分别为 19%和 7%。黑人儿童(危险比[HR],1.21;95%置信区间[CI],1.18-1.24)、其他种族(亚洲、美国印第安人、夏威夷或太平洋岛民、多种族或未报告;HR,1.37;95%CI,1.33-1.40)和拉丁裔儿童(HR,1.65;95%CI,1.60-1.70)的覆盖范围中断风险较高,而白人儿童的覆盖范围中断风险较低。医疗复杂程度较高的儿童(HR,1.15;95%CI,1.12-1.19)的覆盖范围中断风险也更高。居住在失业率最高的县的儿童的覆盖范围中断风险较低(HR,0.89;95%CI,0.85-0.94),并且县一级儿童贫困率和毕业率的比较显示差异很小或没有差异。在包括所有医疗费用的情况下,全人群的估计 PMPM 成本为 125.73 美元。在防止退学的反事实情况下,整个队列的估计 PMPM 成本略低(122.14 美元)。在所有亚组中,在防止退学的情况下,估计的 PMPM 成本略低(2-8 美元)。
在这项队列研究中,医疗补助计划覆盖范围中断的风险很高,许多来自历史上处于边缘地位的社区的合格儿童仍在经历不稳定的入组。除了改善健康结果外,通过减少退学来改善政策覆盖范围差距也可能降低医疗补助计划的成本。