Department of Emergency Medicine, University of Michigan, Ann Arbor.
Institute for Health Metrics and Evaluation, University of Washington, Seattle.
JAMA Health Forum. 2021 Dec 30;2(12):e214359. doi: 10.1001/jamahealthforum.2021.4359. eCollection 2021 Dec.
Uninsured people uniquely rely on the emergency department (ED) for care as they are less likely to have access to lower-cost alternatives. Prior work has demonstrated that most uninsured patients are at risk of catastrophic health expenditure (CHE) after being hospitalized for life-saving care. The risk of CHE for a single treat-and-release ED visit that does not result in a hospitalization among uninsured patient encounters is currently unknown.
To estimate the overall national risk of CHE among uninsured patients after a single treat-and-release ED visit from 2006 through 2017, and to characterize this risk across key traits.
This cross-sectional study is based on a nationally representative sample of hospital-based ED visits between 2006 and 2017 in the United States (US) from the Nationwide Emergency Department Sample (NEDS). It examined outpatient ED visits among uninsured patients.
Risk of CHE for ED care defined as an ED charge that exceeds 40% of one's estimated annual post-subsistence income.
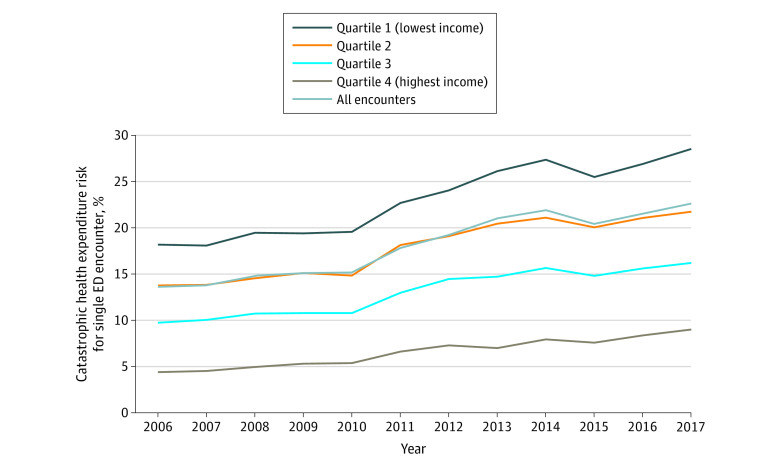
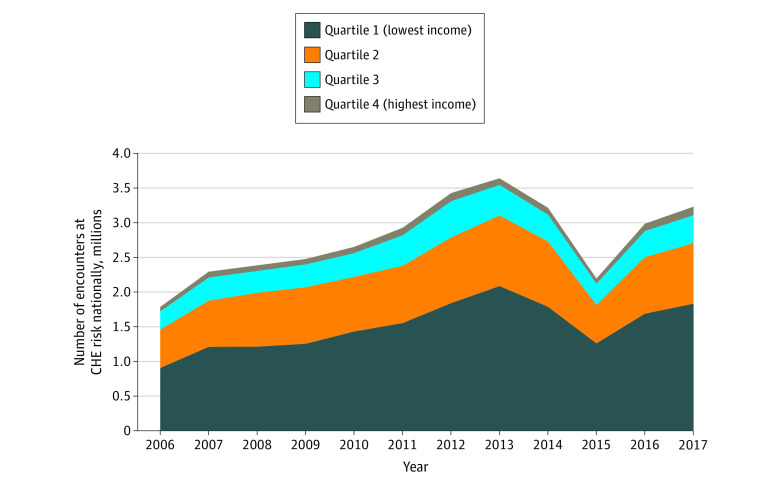
From 2006 to 2017, there were 41.7 million NEDS encounters that met inclusion criteria for this analysis, equating to a nationally weighted estimate of 184.6 million uninsured treat-and-release ED encounters over this period. The median ED charge for a single treat-and-release encounter grew from $842 in 2006 to $2033 by 2017. Approximately 1 in 5 uninsured patients (18% [95% CI, 18.0%-18.0%]) were at risk of CHE for a single treat-and-release ED visit over the study period. This estimated CHE risk increased from 13.6% (95% CI, 13.6%-13.6%) in 2006 to 22.6% (95% CI, 22.6%-22.7%) in 2017. Those living in the lowest income quartile faced a disproportionate share of this risk, with nearly 1 in 3 (28.5% [95% CI, 28.5%-28.6%]) facing CHE risk in 2017. In 2017, an estimated 3.2 million patient encounters nationally were at risk of CHE after a single treat-and-release ED visit.
This cross-sectional analysis from 2006 to 2017 of 184.6 million uninsured treat-and-release visits found that 1 in 5 uninsured patient encounters are at risk for CHE. This risk has grown over time. Future policies designed to improve access for unscheduled care must consider the unique role of the ED as the de facto safety net and ensure that uninsured patients are not at undue risk of financial harm for seeking care.
由于未参保人群获得低成本替代方案的机会较少,因此他们唯一依赖急诊部 (ED) 获得医疗服务。先前的研究表明,大多数未参保患者在因挽救生命而住院治疗后,都面临灾难性医疗支出 (CHE) 的风险。目前尚不清楚未参保患者单次接受治疗后即离院 (TREAT-AND-RELEASE) 的 ED 就诊,是否会导致 CHE。
本研究旨在评估 2006 年至 2017 年期间,未参保患者单次接受治疗后即离院 (TREAT-AND-RELEASE) 的 ED 就诊的全国 CHE 总体风险,并对这一风险在关键特征上的表现进行描述。
设计、设置和人群:这是一项基于美国全国急诊部样本 (NEDS) 的全国代表性样本的横断面研究,研究对象为 2006 年至 2017 年期间在医院进行的 ED 就诊的未参保患者。研究人员分析了未参保患者的门诊 ED 就诊情况。
ED 治疗的 CHE 风险定义为 ED 费用超过估计的个人年度生存后收入的 40%。
2006 年至 2017 年,NEDS 共纳入符合本分析标准的 4170 万例就诊,相当于同期全国范围内未参保患者 1.846 亿次 TREAT-AND-RELEASE ED 就诊的加权估计值。单次 TREAT-AND-RELEASE 就诊的 ED 费用中位数从 2006 年的 842 美元增加到 2017 年的 2033 美元。在研究期间,约有 1/5 的未参保患者 (18% [95% CI,18.0%-18.0%]) 存在单次 TREAT-AND-RELEASE ED 就诊的 CHE 风险。这一估计的 CHE 风险从 2006 年的 13.6% (95% CI,13.6%-13.6%) 增加到 2017 年的 22.6% (95% CI,22.6%-22.7%)。收入最低的四分之一人群面临着不成比例的风险,其中近 1/3 (28.5% [95% CI,28.5%-28.6%]) 在 2017 年面临 CHE 风险。2017 年,全国估计有 320 万例 ED 就诊存在 CHE 风险。
本研究对 2006 年至 2017 年期间 1.846 亿次未参保 TREAT-AND-RELEASE 就诊进行了横断面分析,结果发现,1/5 的未参保患者就诊存在 CHE 风险。这一风险随着时间的推移而增加。未来旨在改善非计划性医疗服务获取机会的政策,必须考虑到 ED 作为事实上的安全网的独特作用,并确保未参保患者不会因寻求医疗服务而面临不必要的经济风险。