From the Department of Anesthesiology and Perioperative Medicine.
Division of Critical Care Medicine.
Anesth Analg. 2022 Sep 1;135(3):501-510. doi: 10.1213/ANE.0000000000006127. Epub 2022 Aug 17.
Anemia is common in critically ill patients and may be exacerbated through phlebotomy-associated iatrogenic blood loss. Differences in phlebotomy practice across patient demographic characteristics, clinical features, and practice environments are unclear. This investigation provides a comprehensive description of contemporary phlebotomy practices for critically ill adults.
This is an observational cohort study of adults ≥18 years of age requiring intensive care unit (ICU) admission between January 1, 2019, and December 31, 2019, at a large academic medical center. Descriptive statistics were utilized to summarize all phlebotomy episodes throughout hospitalization, with each phlebotomy episode defined by unique peripheral venous, central venous, or arterial accesses for laboratory draws, exclusive of finger sticks. Secondarily, financial costs of phlebotomy and the relationships between phlebotomy practices, hemoglobin concentrations, and red blood cell (RBC) transfusions were evaluated.
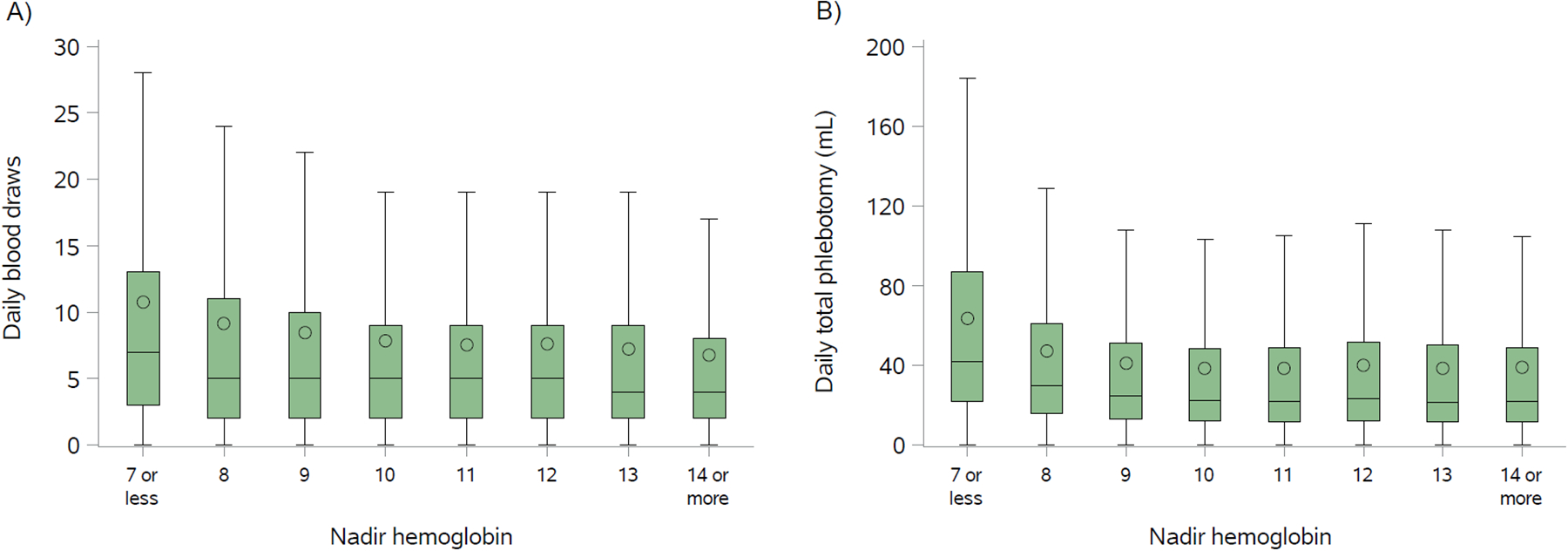
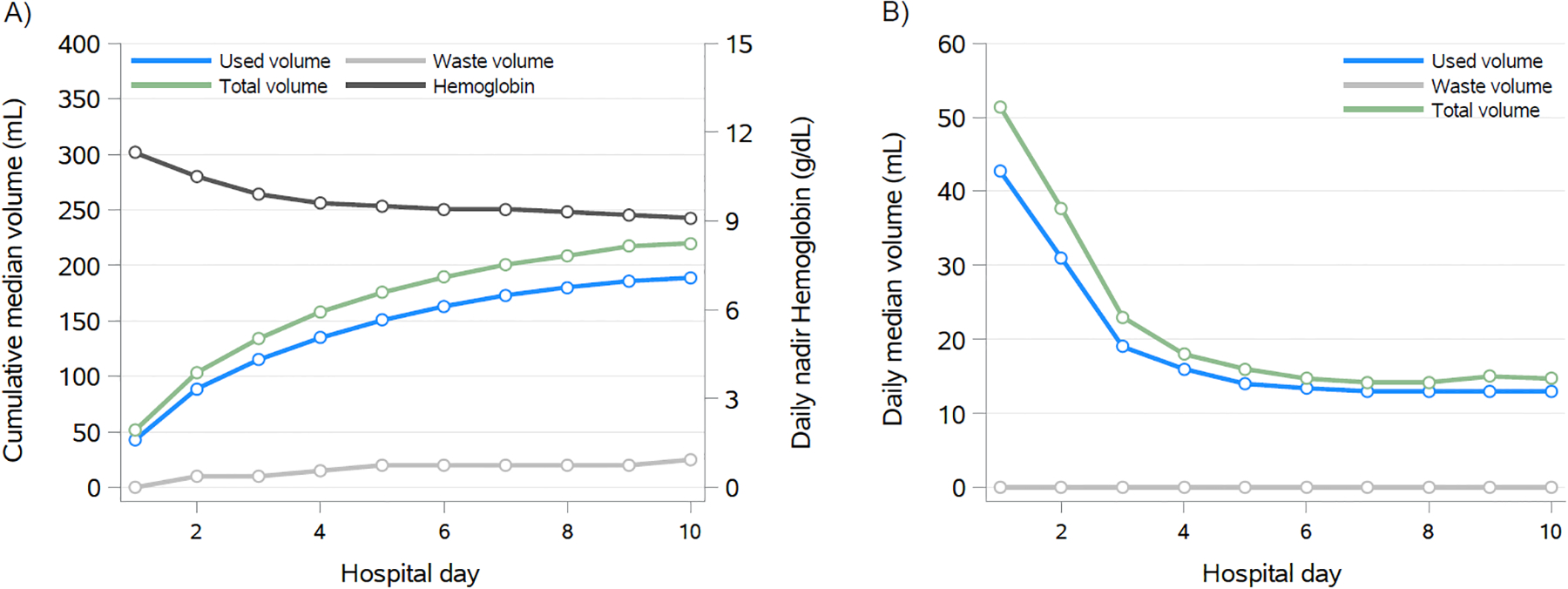
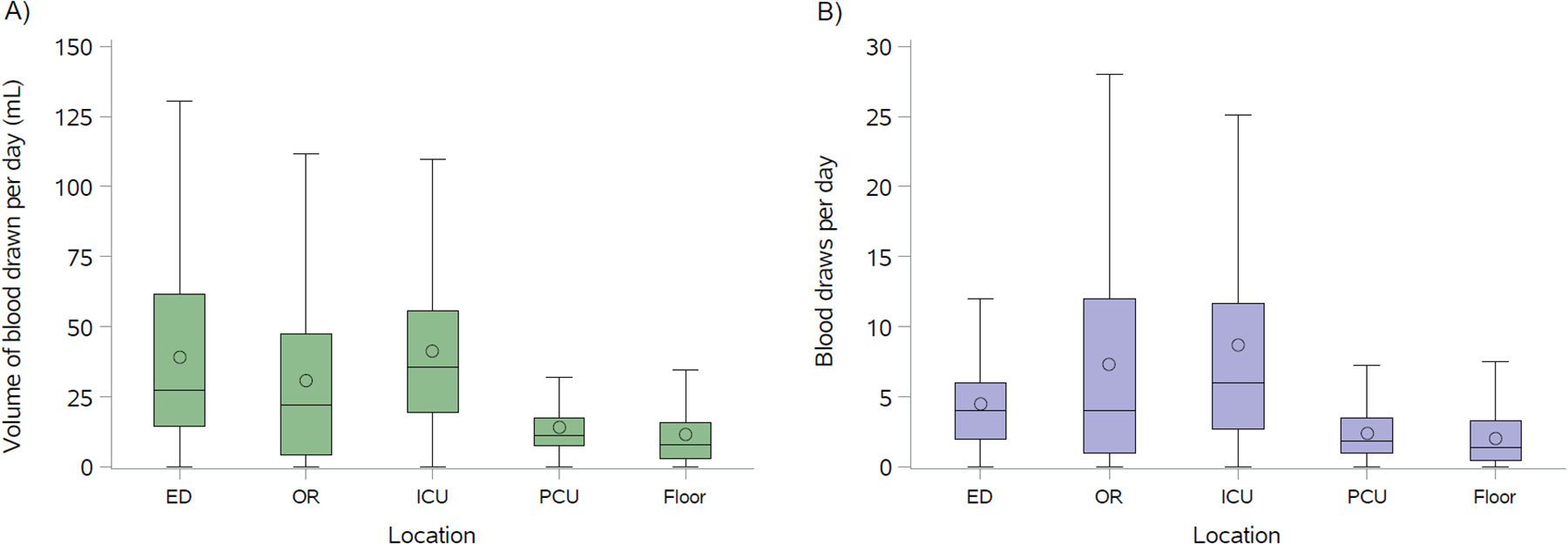
A total of 6194 patients were included: 59% were men with a median (interquartile range) age of 66 (54-76) years and median ICU and hospital durations of 2.1 (1.4-3.9) and 7.1 (4.3-11.8) days, respectively. The median number of unique laboratory draws was 41 (18-88) throughout hospitalization, with a median volume of 232 (121-442) mL, corresponding to 5.2 (2.6-8.8) draws and 29 (19-43) mL per day. Waste (ie, discard) volume was responsible for 10.8% of total phlebotomy volume. Surgical patients had a higher number of phlebotomy episodes and greater total phlebotomy volumes compared to nonsurgical patients. Phlebotomy practices differed across ICU types, with the greatest frequency of laboratory draws in the cardiac surgical ICU and the greatest daily phlebotomy volume in the medical ICU. Across hospitalization, ICU environments had the greatest frequency and volumes of laboratory draws, with the least intensive phlebotomy practice observed in the general hospital wards. Patients in the highest quartile of cumulative blood drawn experienced the longest hospitalizations, lowest nadir hemoglobin concentrations, and greatest RBC transfusion utilization. Differences in phlebotomy practice were limited across patient age, gender, and race. Hemoglobin concentrations declined during hospitalization, congruent with intensity of phlebotomy practice. Each 100 mL of phlebotomy volume during hospitalization was associated with a 1.15 (95% confidence interval [CI], 1.14-1.17; P < .001) multiplicative increase in RBC units transfused in adjusted analyses. Estimated annual phlebotomy costs exceeded $15 million (approximately $2500 per patient admission).
Phlebotomy continues to be a major source of blood loss in hospitalized patients with critical illness, and more intensive phlebotomy practices are associated with lower hemoglobin concentrations and greater transfusion utilization.
贫血在危重症患者中很常见,并且可能因与采血相关的医源性失血而加重。在患者人口统计学特征、临床特征和实践环境方面,采血实践存在差异,目前尚不清楚。本研究全面描述了危重症成人的当代采血实践。
这是一项观察性队列研究,纳入了 2019 年 1 月 1 日至 2019 年 12 月 31 日期间在一家大型学术医疗中心入住重症监护病房(ICU)的年龄≥18 岁的成年人。采用描述性统计方法总结整个住院期间的所有采血事件,每次采血事件均定义为用于实验室采血的独特外周静脉、中心静脉或动脉通路,不包括指尖采血。其次,评估了采血的经济成本以及采血实践、血红蛋白浓度和红细胞(RBC)输注之间的关系。
共纳入 6194 例患者:59%为男性,中位(四分位间距)年龄为 66(54-76)岁,中位 ICU 和住院时间分别为 2.1(1.4-3.9)和 7.1(4.3-11.8)天。整个住院期间,实验室采血的中位数次数为 41(18-88)次,采血量中位数为 232(121-442)mL,相当于每天采血 5.2(2.6-8.8)次和 29(19-43)mL。废物(即丢弃)量占总采血量的 10.8%。与非手术患者相比,手术患者的采血次数更多,总采血量更大。不同 ICU 类型的采血实践存在差异,心脏外科 ICU 的实验室采血频率最高,内科 ICU 的每日采血量最大。整个住院期间,ICU 环境的实验室采血频率和采血量最高,而普通病房的采血实践最少。在累积采血量最高的四分位数患者中,住院时间最长,最低的血红蛋白浓度最低,RBC 输注使用率最高。患者的年龄、性别和种族差异对采血实践的影响有限。血红蛋白浓度在住院期间下降,与采血实践的强度一致。在住院期间每 100 mL 采血量与 RBC 单位输注量的增加呈 1.15(95%置信区间[CI],1.14-1.17;P<0.001)的倍增关系。校正分析表明,每年的采血费用估计超过 1500 万美元(约 2500 美元/患者入院)。
采血仍然是危重症住院患者失血的主要来源,更密集的采血实践与更低的血红蛋白浓度和更大的输血利用率相关。