Kuroda Hidekatsu, Oikawa Takayoshi, Ninomiya Masashi, Fujita Masashi, Abe Kazumichi, Okumoto Kazuo, Katsumi Tomohiro, Sato Wataru, Igarashi Go, Iino Chikara, Endo Tetsu, Tanabe Nobukazu, Numao Hiroshi, Fukuda Shinsaku, Iijima Katsunori, Masamune Atsushi, Ohira Hiromasa, Ueno Yoshiyuki, Takikawa Yasuhiro
Division of Hepatology, Department of Internal Medicine, Iwate Medical University, Iwate, Japan.
Division of Gastroenterology, Tohoku University Graduate School of Medicine, Sendai, Japan.
Liver Cancer. 2022 Feb 15;11(4):383-396. doi: 10.1159/000522424. eCollection 2022 Jul.
There is limited information regarding the benefits of Lenvatinib-transcatheter arterial chemoembolization (LEN-TACE) sequential therapy for unresectable hepatocellular carcinoma (u-HCC). We compared the efficacy and safety of LEN-TACE sequential therapy to LEN monotherapy and investigated the factors contributing to the LEN-TACE sequential therapy deep response.
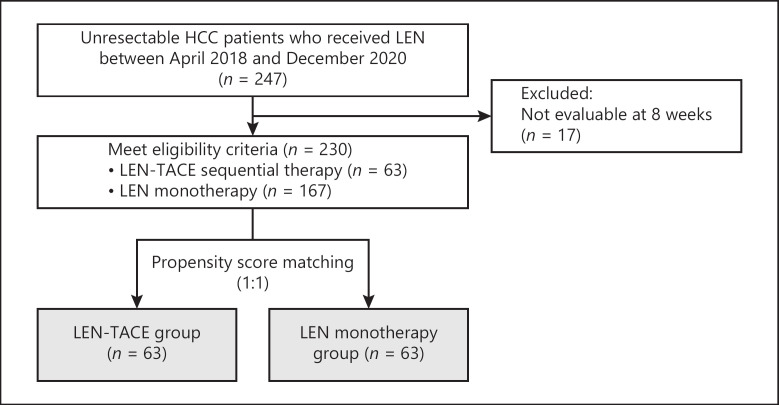
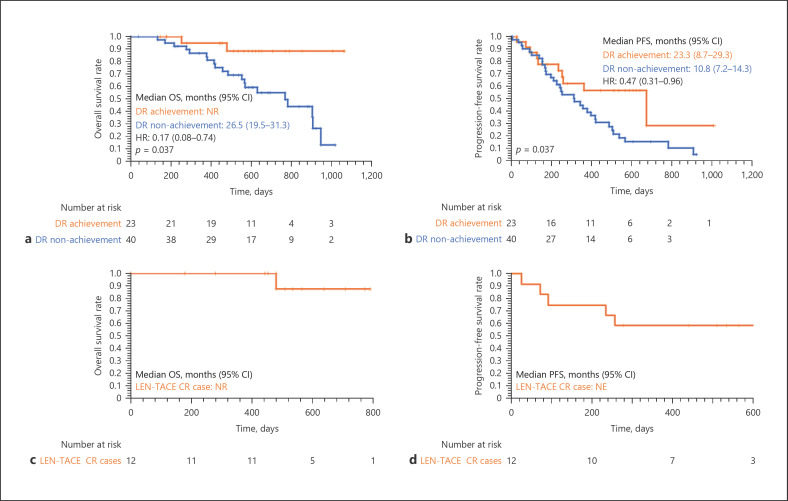
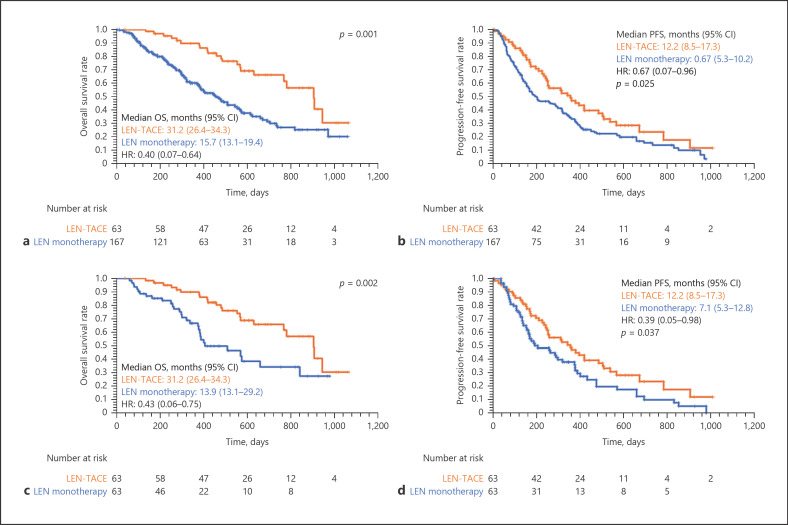
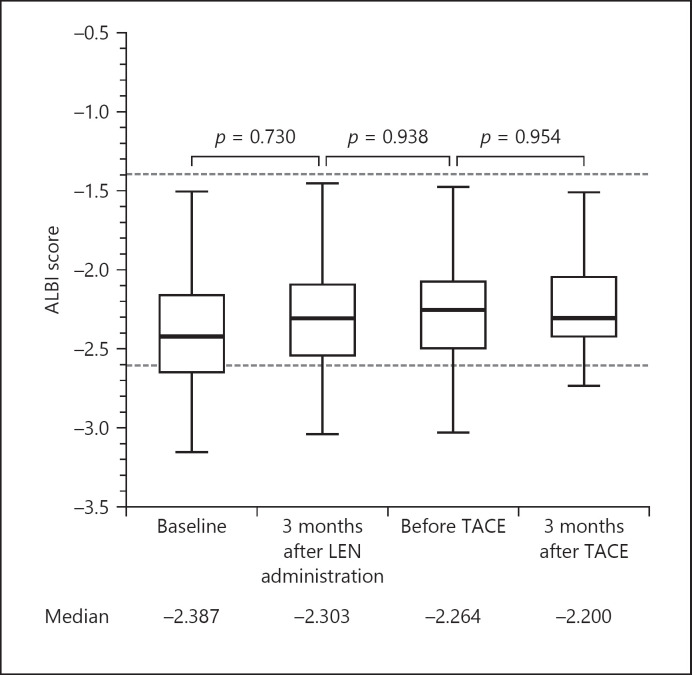
We enrolled a multicenter cohort of 247 patients with u-HCC treated with LEN between 2018 and 2020. Propensity score matching identified 63 matching pairs of patients with well-balanced characteristics. We retrospectively compared the clinical outcomes, including overall survival (OS), progression-free survival (PFS), and incidence of adverse events (AEs), between the LEN-TACE and LEN monotherapy groups. Additionally, we evaluated the tumor response, change in albumin-bilirubin (ALBI) score, factors affecting PFS and OS, and independent predictors contributing to the LEN-TACE sequential therapy deep response. In this study, at eight weeks after resumption of LEN after initial TACE, "deep response" was defined as achieving complete response or partial response (PR) on modified Response Evaluation Criteria in Solid Tumors (mRECIST), and at least a 30% decrease in the sum of diameters of target lesions, taking the baseline sum diameters as the reference.
The OS and PFS in the LEN-TACE group were significantly higher than those in the LEN monotherapy group ( = 0.002 and = 0.037, respectively). The incidence of AEs related to LEN was not significantly different between the two groups. In LEN-TACE sequential therapy, the objective response rate was 61.9%, and the disease control rate was 74.6%, according to the mRECIST criteria. No significant change in the ALBI score was observed during sequential LEN-TACE therapy. Multivariable analyses revealed that deep response was independently associated with the outcome of the initial response to LEN by mRECIST: PR (odds ratio: 5.176, 95% confidence interval: 1.528-17.537, < 0.001).
LEN-TACE sequential therapy may provide more clinical benefits than LEN monotherapy in u-HCC patients who responded to initial LEN treatment. Objective response according to mRECIST to initial LEN is an independent factor contributing to LEN-TACE sequential therapy deep response.
关于乐伐替尼经动脉化疗栓塞术(LEN-TACE)序贯疗法治疗不可切除肝细胞癌(u-HCC)的益处,相关信息有限。我们比较了LEN-TACE序贯疗法与乐伐替尼单药治疗的疗效和安全性,并研究了促成LEN-TACE序贯疗法深度缓解的因素。
我们纳入了一个多中心队列,其中247例u-HCC患者在2018年至2020年间接受了乐伐替尼治疗。倾向评分匹配确定了63对特征均衡的匹配患者。我们回顾性比较了LEN-TACE组和乐伐替尼单药治疗组的临床结局,包括总生存期(OS)、无进展生存期(PFS)和不良事件(AE)发生率。此外,我们评估了肿瘤反应、白蛋白-胆红素(ALBI)评分变化、影响PFS和OS的因素,以及促成LEN-TACE序贯疗法深度缓解的独立预测因素。在本研究中,在初始TACE后恢复乐伐替尼治疗8周时,“深度缓解”定义为根据实体瘤改良反应评估标准(mRECIST)达到完全缓解或部分缓解(PR),且以基线直径总和为参考,目标病灶直径总和至少减少30%。
LEN-TACE组的OS和PFS显著高于乐伐替尼单药治疗组(分别为 = 0.002和 = 0.037)。两组之间与乐伐替尼相关的AE发生率无显著差异。根据mRECIST标准,在LEN-TACE序贯疗法中,客观缓解率为61.9%,疾病控制率为74.6%。在LEN-TACE序贯治疗期间,未观察到ALBI评分有显著变化。多变量分析显示,深度缓解与mRECIST评估的乐伐替尼初始反应结果独立相关:PR(比值比:5.176,95%置信区间:1.528 - 17.537,< 0.001)。
对于对初始乐伐替尼治疗有反应的u-HCC患者,LEN-TACE序贯疗法可能比乐伐替尼单药治疗提供更多临床益处。根据mRECIST对初始乐伐替尼的客观反应是促成LEN-TACE序贯疗法深度缓解的独立因素。