Department of Radiology, Functional and Molecular Imaging Key Laboratory of Sichuan Province, West China Hospital, Sichuan University, Chengdu, Sichuan, People's Republic of China.
Department of Minimal invasive intervention, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-sen University Cancer Center.
Int J Surg. 2024 Sep 1;110(9):5672-5684. doi: 10.1097/JS9.0000000000001752.
Surgical resection (SR) following transarterial chemoembolization (TACE)-based downstaging is a promising treatment for unresectable hepatocellular carcinoma (uHCC), and identification of patients at high-risk of postoperative recurrence may assist individualized treatment.
To develop and externally validate preoperative and postoperative prognostic models integrating multimodal CT and digital subtraction angiography features as well as clinico-therapeutic-pathological features for predicting disease-free survival (DFS) after TACE-based downstaging therapy.
From March 2008 to August 2022, 488 consecutive patients with Barcelona Clinic Liver Cancer (BCLC) A/B uHCC receiving TACE-based downstaging therapy and subsequent SR were included from four tertiary-care hospitals. All CT and digital subtraction angiography images were independently evaluated by two blinded radiologists. In the derivation cohort ( n =390), the XGBoost algorithm was used for feature selection, and Cox regression analysis for developing nomograms for DFS (time from downstaging to postoperative recurrence or death). In the external testing cohort ( n =98), model performances were compared with five major staging systems.
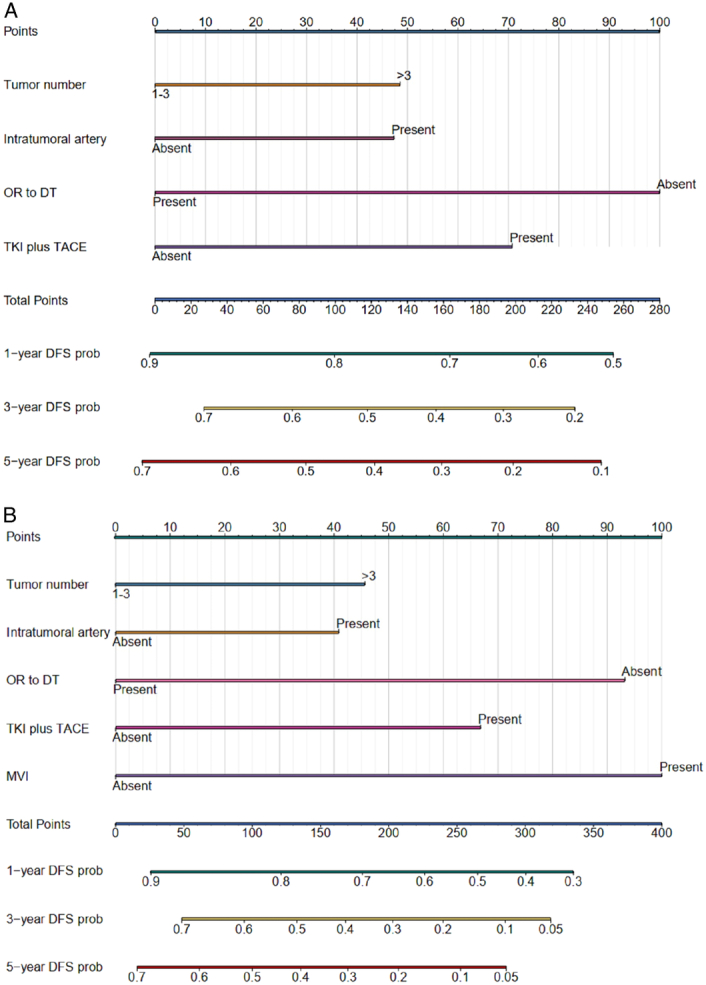
The preoperative nomogram included over three tumors [hazard ratio (HR), 1.42; P =0.003], intratumoral artery (HR, 1.38; P =0.006), TACE combined with tyrosine kinase inhibitor (HR, 0.46; P <0.001) and objective response to downstaging therapy (HR, 1.60; P <0.001); while the postoperative nomogram included over three tumors (HR, 1.43; P =0.013), intratumoral artery (HR, 1.38; P =0.020), TACE combined with tyrosine kinase inhibitor (HR, 0.48; P <0.001), objective response to downstaging therapy (HR, 1.69; P <0.001) and microvascular invasion (HR, 2.20; P <0.001). The testing dataset C-indexes of the preoperative (0.651) and postoperative (0.687) nomograms were higher than all five staging systems (0.472-0.542; all P <0.001). Two prognostically distinct risk strata were identified according to these nomograms (all P <0.001).
Based on 488 patients receiving TACE-based downstaging therapy and subsequent SR for BCLC A/B uHCCs, the authors developed and externally validated two nomograms for predicting DFS, with superior performances than five major staging systems and effective survival stratification.
经动脉化疗栓塞(TACE)降期后手术切除(SR)是治疗不可切除肝细胞癌(uHCC)的一种有前途的方法,识别术后复发风险较高的患者可能有助于个体化治疗。
开发并外部验证术前和术后预测 TACE 降期治疗后无病生存(DFS)的预测模型,该模型整合了多模态 CT 和数字减影血管造影特征以及临床治疗病理特征。
从 2008 年 3 月至 2022 年 8 月,从四家三级医院共纳入 488 例巴塞罗那临床肝癌(BCLC)A/B 期 uHCC 患者,接受 TACE 降期治疗和随后的 SR。所有 CT 和数字减影血管造影图像均由两名盲法放射科医生独立评估。在推导队列(n=390)中,使用 XGBoost 算法进行特征选择,使用 Cox 回归分析建立 DFS(从降期到术后复发或死亡的时间)的列线图。在外部测试队列(n=98)中,将模型性能与五个主要分期系统进行比较。
术前列线图包括超过三个肿瘤[风险比(HR),1.42;P=0.003]、肿瘤内动脉(HR,1.38;P=0.006)、TACE 联合酪氨酸激酶抑制剂(HR,0.46;P<0.001)和降期治疗的客观反应(HR,1.60;P<0.001);而术后列线图包括超过三个肿瘤(HR,1.43;P=0.013)、肿瘤内动脉(HR,1.38;P=0.020)、TACE 联合酪氨酸激酶抑制剂(HR,0.48;P<0.001)、降期治疗的客观反应(HR,1.69;P<0.001)和微血管侵犯(HR,2.20;P<0.001)。测试数据集术前(0.651)和术后(0.687)列线图的 C 指数均高于五个分期系统(0.472-0.542;均 P<0.001)。根据这些列线图确定了两个具有不同预后的风险分层(均 P<0.001)。
基于 488 例接受 TACE 降期治疗和随后 SR 治疗的 BCLC A/B uHCC 患者,作者开发并外部验证了两个预测 DFS 的列线图,其性能优于五个主要分期系统,并能有效进行生存分层。