Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan.
Cardiovascular Research Center, National Yang-Ming Chiao Tung University, Taipei, Taiwan.
PLoS One. 2022 Aug 18;17(8):e0272258. doi: 10.1371/journal.pone.0272258. eCollection 2022.
Acute infection is a well-known provocative factor of acute myocardial infarction (AMI). Prognosis is worse when it is associated with sepsis. Coronary revascularization is reported to provide benefit in these patients; however, the optimal timing remains uncertain.
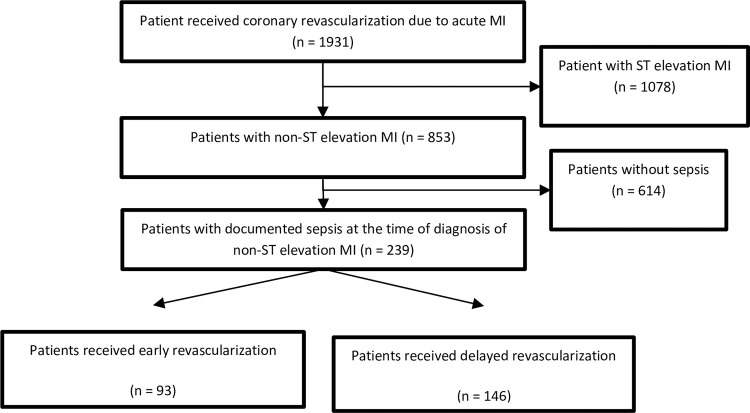
This retrospective study was performed at a tertiary center in Taipei from January 2010 to December 2017. 1931 patients received coronary revascularization indicated for AMI. Among these, 239 patients were hospitalized for acute infection but later developed AMI. Patients with either an ST-elevation myocardial infarct or the absence of obstructive coronary artery disease were excluded. Revascularization was performed via either percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG). We defined early and delayed revascularization groups if it was performed within or after 24 hours of the diagnosis of AMI, respectively. We evaluated whether the timing of revascularization altered 30-day and one-year all-cause mortality.
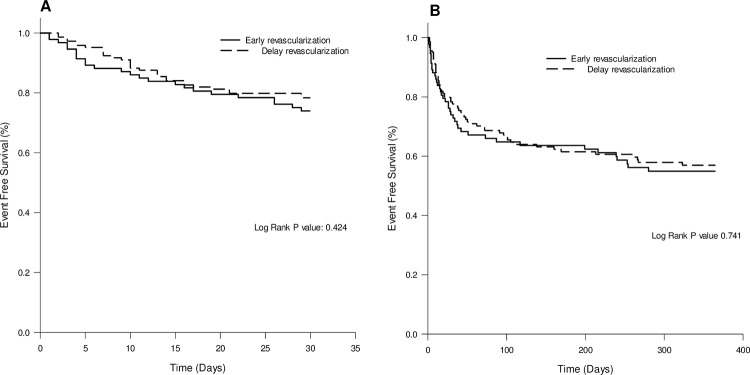
At one month, 24 (26%) patients died in early revascularization group and 32 (22%) patients in delayed revascularization group. At one year, 40 (43%) and 59 (40%) patients died on early and delayed revascularization groups respectively. Early revascularization did not result in lower 30-day all-cause mortality (P = 0.424), and one-year all-cause mortality (Hazard ratio (HR): 0.935; 95% confidence interval (CI): 0.626-1.397, P = 0.742) than delay revascularization.
Timing of coronary revascularization of post infectious acute coronary syndrome may be arranged according to individual risk category as those without sepsis.
急性感染是急性心肌梗死(AMI)的已知诱发因素。当它与败血症相关时,预后更差。据报道,冠状动脉血运重建可为这些患者带来益处;然而,最佳时机仍不确定。
本回顾性研究于 2010 年 1 月至 2017 年 12 月在台北的一家三级中心进行。1931 例患者因 AMI 接受了冠状动脉血运重建。其中,239 例患者因急性感染住院,但后来发生 AMI。排除 ST 段抬高型心肌梗死或无阻塞性冠状动脉疾病的患者。血运重建通过经皮冠状动脉介入治疗(PCI)或冠状动脉旁路移植术(CABG)进行。如果在 AMI 诊断后 24 小时内或之后进行血运重建,则定义为早期和延迟血运重建组。我们评估了血运重建时机是否改变了 30 天和 1 年的全因死亡率。
在一个月时,早期血运重建组有 24 例(26%)患者死亡,延迟血运重建组有 32 例(22%)患者死亡。在一年时,早期和延迟血运重建组分别有 40 例(43%)和 59 例(40%)患者死亡。早期血运重建并未降低 30 天全因死亡率(P=0.424),也未降低 1 年全因死亡率(风险比(HR):0.935;95%置信区间(CI):0.626-1.397,P=0.742),低于延迟血运重建。
对于无败血症的患者,可根据个体风险类别安排感染后急性冠状动脉综合征的冠状动脉血运重建时机。