Department of Clinical Epidemiology and Health Economics, School of Public Health, and.
Data Science Centre, Jichi Medical University, Shimotsuke, Tochigi, Japan.
Ann Am Thorac Soc. 2023 Jan;20(1):102-109. doi: 10.1513/AnnalsATS.202206-475OC.
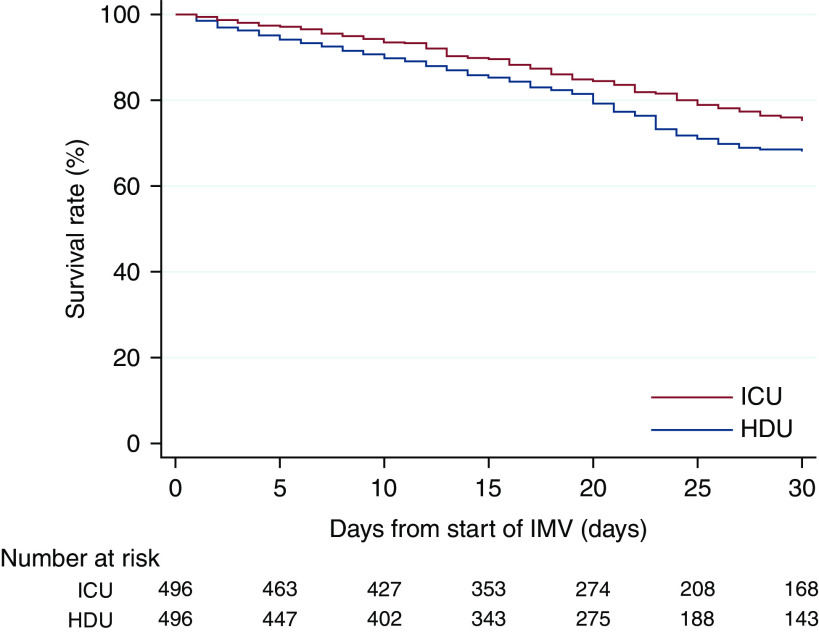
High-dependency care units (HDUs), also termed "intermediate care units", "step-down units", or "respiratory HDUs", are areas in which degrees of patient care and costs are between those of the intensive care unit (ICU) and the general ward. In general, patients requiring mechanical ventilation are treated in the ICU rather than in the HDU, except for the use of HDU beds as surge capacity beds during a massive strain; however, the HDU, as well as ICU, are used as the standard care units for mechanically ventilated patients with coronavirus disease (COVID-19) in Japan. To assess the outcomes of patients with COVID-19 with invasive mechanical ventilation treated in the HDU versus those treated in the ICU. In this retrospective cohort study, we used a multicenter inpatient database in Japan to identify mechanically ventilated patients with COVID-19 in the ICU or HDU on the start day of invasive mechanical ventilation from February 10, 2020, to November 30, 2021. The primary outcome was in-hospital mortality within 30 days from the start of the first invasive mechanical ventilation. Propensity score matching was performed to compare the outcomes of patients treated in the ICU with those treated in the HDU. Of 1,985 eligible patients with COVID-19 with invasive mechanical ventilation, 1,303 (66%) were treated in the ICU, and 682 (34%) were treated in the HDU on the start day of invasive mechanical ventilation. After propensity score matching, patients treated in the ICU had significantly lower in-hospital mortality within 30 days than those treated in the HDU (18.3% vs. 24.2%; risk difference, -5.8%; 95% confidence interval, -10.9% to -0.8%). This multicenter observational study in Japan suggests that care for mechanically ventilated patients with COVID-19 in the ICU may significantly reduce in-hospital mortality within 30 days compared with care in the HDU. Establishing a critical care system that would allow patients with COVID-19 requiring ventilators to be treated in the ICU is desirable. Because this study was an observational study, our finding represents an association, not causation. Further studies of different critical care systems are warranted to confirm our findings.
高依赖护理单元(HDU),也称为“中级护理单元”、“下调节单元”或“呼吸 HDU”,是指患者护理和成本介于重症监护病房(ICU)和普通病房之间的区域。一般来说,需要机械通气的患者在 ICU 接受治疗,而不是在 HDU 接受治疗,除非在大规模压力下使用 HDU 床位作为应急能力床位;然而,HDU 以及 ICU,都被用作日本患有冠状病毒病(COVID-19)需要机械通气的患者的标准护理单元。评估在 HDU 接受治疗的 COVID-19 合并有创机械通气患者与在 ICU 接受治疗的患者的结局。在这项回顾性队列研究中,我们使用日本的一个多中心住院患者数据库,确定了 2020 年 2 月 10 日至 2021 年 11 月 30 日有创机械通气开始日当天在 ICU 或 HDU 接受机械通气的 COVID-19 患者。主要结局是首次有创机械通气开始后 30 天内的院内死亡率。进行倾向评分匹配以比较在 ICU 接受治疗的患者与在 HDU 接受治疗的患者的结局。在 1985 名符合条件的 COVID-19 合并有创机械通气患者中,1303 名(66%)在 ICU 接受治疗,682 名(34%)在有创机械通气开始日在 HDU 接受治疗。在进行倾向评分匹配后,与在 HDU 接受治疗的患者相比,在 ICU 接受治疗的患者 30 天内院内死亡率显著降低(18.3%比 24.2%;风险差异,-5.8%;95%置信区间,-10.9%至-0.8%)。这项在日本进行的多中心观察性研究表明,与在 HDU 接受治疗相比,在 ICU 为 COVID-19 合并机械通气的患者提供护理可能会显著降低 30 天内的院内死亡率。建立一个能够让需要呼吸机的 COVID-19 患者在 ICU 接受治疗的重症监护系统是可取的。由于这项研究是一项观察性研究,我们的发现代表一种关联,而不是因果关系。需要进一步研究不同的重症监护系统来证实我们的发现。