Pediatric Intensive Care Unit, Meyer Children's University Hospital, Viale Pieraccini 24, 50139, Florence, Italy.
Section of Anesthesiology and Intensive Care, Department of Health Sciences, University of Florence, Florence, Italy.
Intensive Care Med. 2022 Oct;48(10):1397-1408. doi: 10.1007/s00134-022-06810-1. Epub 2022 Aug 19.
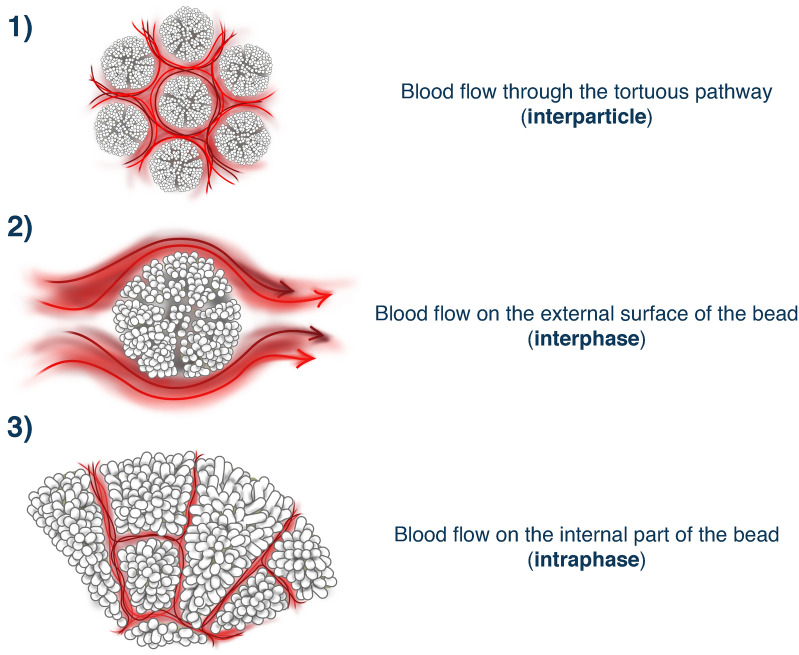
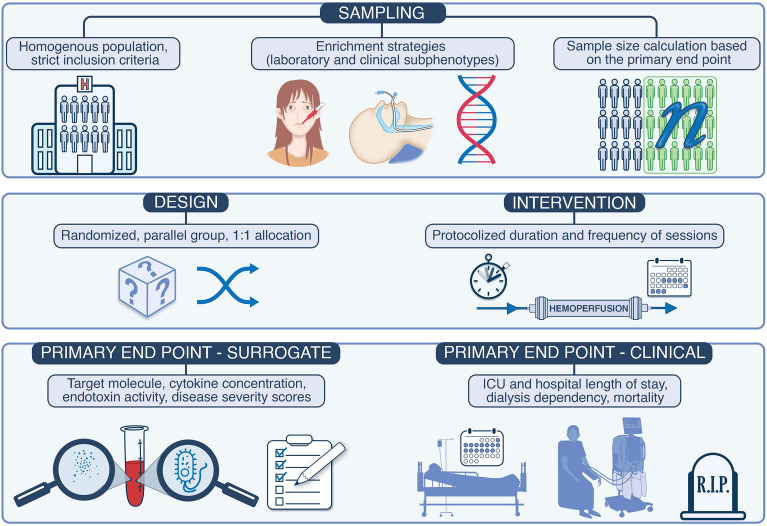
Multiple organ failure following a septic event derives from immune dysregulation. Many of the mediators of this process are humoral factors (cytokines), which could theoretically be cleared by direct adsorption through a process called hemoperfusion. Hemoperfusion through devices, which bind specific molecules like endotoxin or theoretically provide non-specific adsorption of pro-inflammatory mediators has been attempted and studied for several decades with variable results. More recently, technological evolution has led to the increasing application of adsorption due to more biocompatible and possibly more efficient biomaterials. As a result, new indications are developing in this field, and novel tools are available for clinical use. This narrative review will describe current knowledge regarding technical concepts, safety, and clinical results of hemoperfusion. Finally, it will focus on the most recent literature regarding adsorption applied in critically ill patients and their indications, including recent randomized controlled trials and future areas of investigation. Clinical trials for the assessment of efficacy of hemoperfusion in septic patients should apply the explanatory approach. This includes a highly selected homogenous patient population. Enrichment criteria such as applying genetic signature and molecular biomarkers allows the identification of subphenotypes of patients. The intervention must be delivered by a multidisciplinary team of trained personnel. The aim is to maximize the signals for efficacy and safety. In a homogenous cohort, confounding uncontrolled variables are less likely to exist. Trials with highly selected populations have a high internal validity but poor generalizability. The parallel design described in the figure is robust and usually is required by regulatory agencies for the approval of a new treatment. Allocation concealment and randomization are key to minimize bias such as confirmation bias, observer bias. The intervention should be delivered following a strict protocol. Deviations from the protocol might negatively influence the potential effects of the therapies. Surrogates such as cytokine measurement are adequate primary outcomes in phase 3 trials with small sample size because there is a higher likelihood of finding positive results concerning surrogate markers than in respect with clinical outcomes. Once a trial shows positive results concerning surrogate markers, a rationale for another phase 3 trial exploring clinical outcomes is built, justifying the allocation of financial sources to the intended trial.
在感染性事件后发生的多器官衰竭源于免疫失调。这个过程中的许多介质是体液因子(细胞因子),理论上可以通过称为血液灌流的过程直接吸附清除。几十年来,已经尝试并研究了通过设备进行血液灌流,这些设备可以结合特定分子(如内毒素),或者理论上提供促炎介质的非特异性吸附,但其结果各不相同。最近,技术的发展导致越来越多地应用吸附,因为这可以提高生物相容性和可能的效率。因此,该领域正在出现新的适应症,并且有新的工具可供临床使用。本叙述性综述将描述血液灌流的技术概念、安全性和临床结果的最新知识。最后,它将重点介绍最近关于在危重症患者中应用吸附的文献及其适应症,包括最近的随机对照试验和未来的研究领域。评估血液灌流在脓毒症患者中的疗效的临床试验应采用解释性方法。这包括高度选择的同质患者人群。富集标准,如应用遗传特征和分子生物标志物,允许识别患者的亚表型。干预措施必须由经过培训的多学科团队提供。目的是最大限度地提高疗效和安全性的信号。在同质队列中,不太可能存在混杂的未控制变量。具有高度选择人群的试验具有较高的内部有效性,但推广性较差。图中描述的平行设计是稳健的,通常是监管机构批准新治疗方法所必需的。分配隐藏和随机化是减少确认偏倚、观察偏倚等偏倚的关键。干预措施应严格按照方案进行。偏离方案可能会对潜在治疗效果产生负面影响。在样本量较小的 3 期试验中,替代物如细胞因子测量是足够的主要结局,因为与临床结局相比,替代标志物的阳性结果更有可能出现。一旦试验显示替代标志物的阳性结果,就可以构建另一个探索临床结局的 3 期试验的理由,为预期试验分配资金来源。