Department of Hematology and Rheumatology, Faculty of Medicine, Kindai University, Osaka, Sayama, Japan.
Eli Lilly Japan K.K, Kobe, Japan.
Adv Ther. 2022 Oct;39(10):4792-4807. doi: 10.1007/s12325-022-02258-3. Epub 2022 Aug 19.
Treatment options in patients with mantle cell lymphoma (MCL) failing ibrutinib are limited, with no standard therapies defined. This study aimed to investigate real-world treatment patterns and outcomes for patients with MCL following ibrutinib.
This study utilized a de-identified hospital-based claims database (Medical Data Vision) in Japan. Eligible patients were adults who were diagnosed with MCL and had received antitumor drugs between December 2010 and July 2020. Patients were followed from the first antitumor drug treatment until the end of available data up to July 2021. Time-to-event analyses utilized the Kaplan-Meier method. Factors for receiving post-ibrutinib therapy were explored with logistic regression analysis.
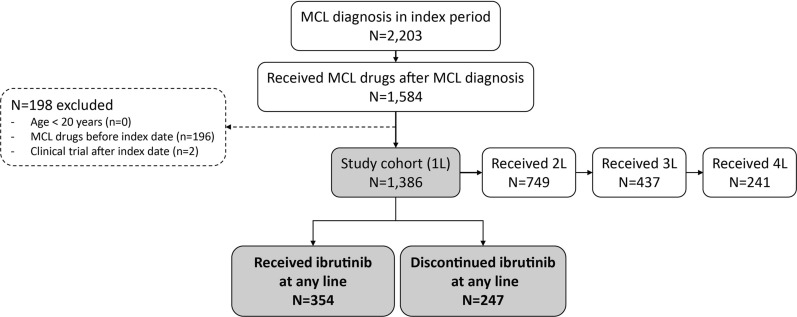
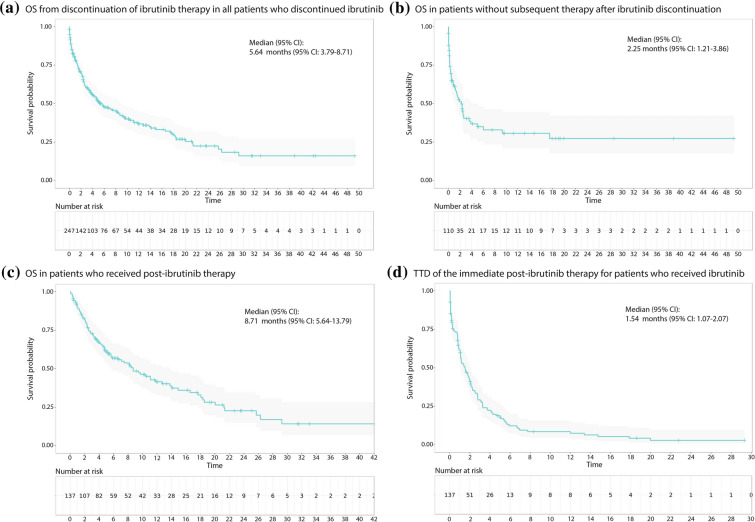
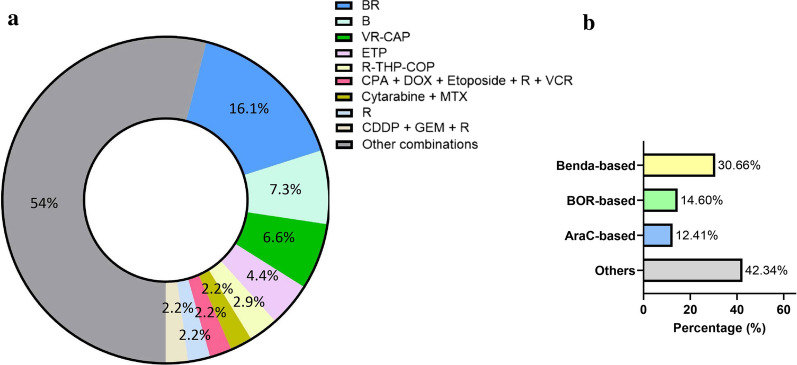
Of the 1386 patients who started antitumor drug therapy, 247 patients received and discontinued ibrutinib at any line of therapy. Among them, 137 patients (55.5%) received subsequent therapy. The median age at the end of ibrutinib therapy was 77 (range 42-95), and 44 patients had a dependent activity of daily living (ADL). Factors negatively associated with receiving post-ibrutinib therapy after discontinuation of ibrutinib were age ≥ 75 years (odds ratio [95% CI] 0.46 [0.26-0.80]) and emergency hospital admissions (0.37 [0.17-0.84]). Immediate post-ibrutinib therapy regimens were highly diverse, with BR (bendamustine, rituximab) only prescribed in more than 10% of patients. The median duration of post-ibrutinib therapy was 1.5 months (95% CI 1.07-2.07). The median overall survival from the end of ibrutinib therapy in patients regardless of the receipt of post-ibrutinib therapy (n = 247), in those who did not receive post-ibrutinib therapy (n = 110), and in those who received post-ibrutinib therapy (n = 137) was 5.6 months (95% CI 3.8-8.7), 2.3 months (95% CI 1.2-3.9), and 8.7 months (95% CI 5.6-13.8), respectively. The most common adverse event during post-ibrutinib therapy was infection, with the use of anti-infectives (17%).
Patients with MCL previously treated with ibrutinib have poor ability to carry out ADL and experience very poor outcomes. New safe, effective therapies are needed.
伊布替尼治疗失败的套细胞淋巴瘤(MCL)患者的治疗选择有限,尚无标准疗法。本研究旨在调查伊布替尼治疗后 MCL 患者的真实世界治疗模式和结局。
本研究利用了日本一个去标识的基于医院的索赔数据库(Medical Data Vision)。符合条件的患者为接受抗肿瘤药物治疗的成年 MCL 患者,治疗时间为 2010 年 12 月至 2020 年 7 月。患者从第一次抗肿瘤药物治疗开始随访,直到 2021 年 7 月可获得数据的截止日期。使用 Kaplan-Meier 方法进行生存时间分析。采用逻辑回归分析探讨接受伊布替尼治疗后治疗的因素。
在开始抗肿瘤药物治疗的 1386 名患者中,有 247 名患者在任何治疗线均接受并停用了伊布替尼。其中,有 137 名患者(55.5%)接受了后续治疗。伊布替尼治疗结束时的中位年龄为 77 岁(范围为 42-95),44 名患者日常生活活动能力(ADL)依赖。与停用伊布替尼后接受伊布替尼治疗后相关的负面因素是年龄≥75 岁(优势比[95%置信区间]0.46 [0.26-0.80])和紧急住院治疗(0.37 [0.17-0.84])。伊布替尼治疗后即刻治疗方案高度多样化,BR(苯达莫司汀、利妥昔单抗)仅在超过 10%的患者中处方。伊布替尼治疗后治疗的中位持续时间为 1.5 个月(95%置信区间 1.07-2.07)。在无论是否接受伊布替尼治疗后(n=247)、未接受伊布替尼治疗后(n=110)和接受伊布替尼治疗后(n=137)的伊布替尼治疗结束时,患者的中位总生存期为 5.6 个月(95%置信区间 3.8-8.7)、2.3 个月(95%置信区间 1.2-3.9)和 8.7 个月(95%置信区间 5.6-13.8)。伊布替尼治疗后最常见的不良事件是感染,使用了抗感染药物(17%)。
先前接受伊布替尼治疗的 MCL 患者 ADL 能力差,预后极差。需要新的安全有效的治疗方法。