Department of Molecular Medicine and Surgery, Karolinska Institutet, Colorectal Surgery Unit, Karolinska University Hospital, Anna Steckséns gata 30A D2:05, 171 76, Solna Stockholm, Sweden.
Medical Unit of Trauma, Emergency Surgery and Orthopaedics, Karolinska University Hospital, Stockholm, Sweden.
BMC Cancer. 2022 Aug 19;22(1):907. doi: 10.1186/s12885-022-10005-8.
Only a limited proportion of patients with metastatic colorectal cancer (mCRC) receives metastatic surgery (including local ablative therapy). The aim was to investigate whether hospital volume and hospital level were associated with the chance of metastatic surgery.
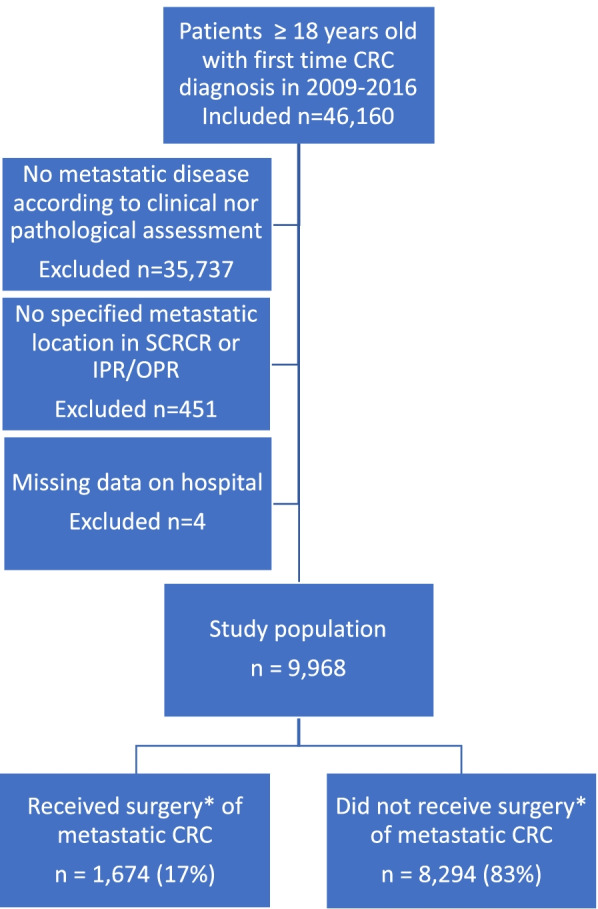
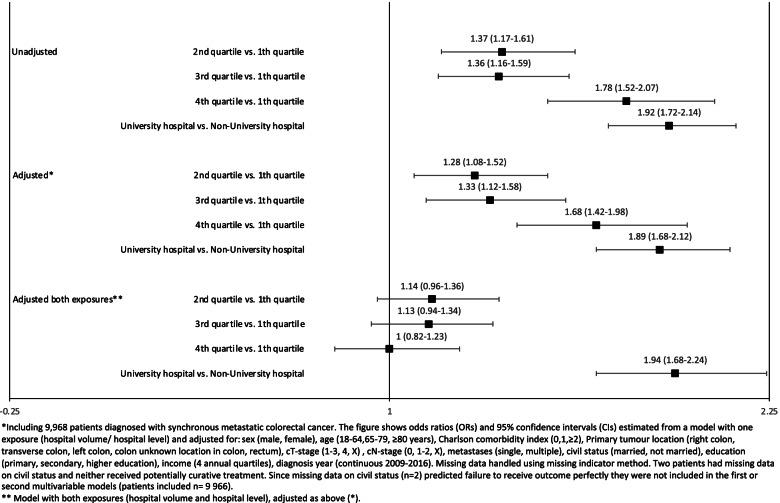
This national cohort retrieved from the CRCBaSe linkage included all Swedish adult patients diagnosed with synchronous mCRC in 2009-2016. The association between annual hospital volume of incident mCRC patients and the chance of metastatic surgery, and survival, were assessed using logistic regression and Cox regression models, respectively. Hospital level (university/non-university) was evaluated as a secondary exposure in a similar manner. Both uni- and multivariable (adjusted for sex, age, Charlson comorbidity index, year of diagnosis, cancer characteristics and socioeconomic factors) models were fitted.
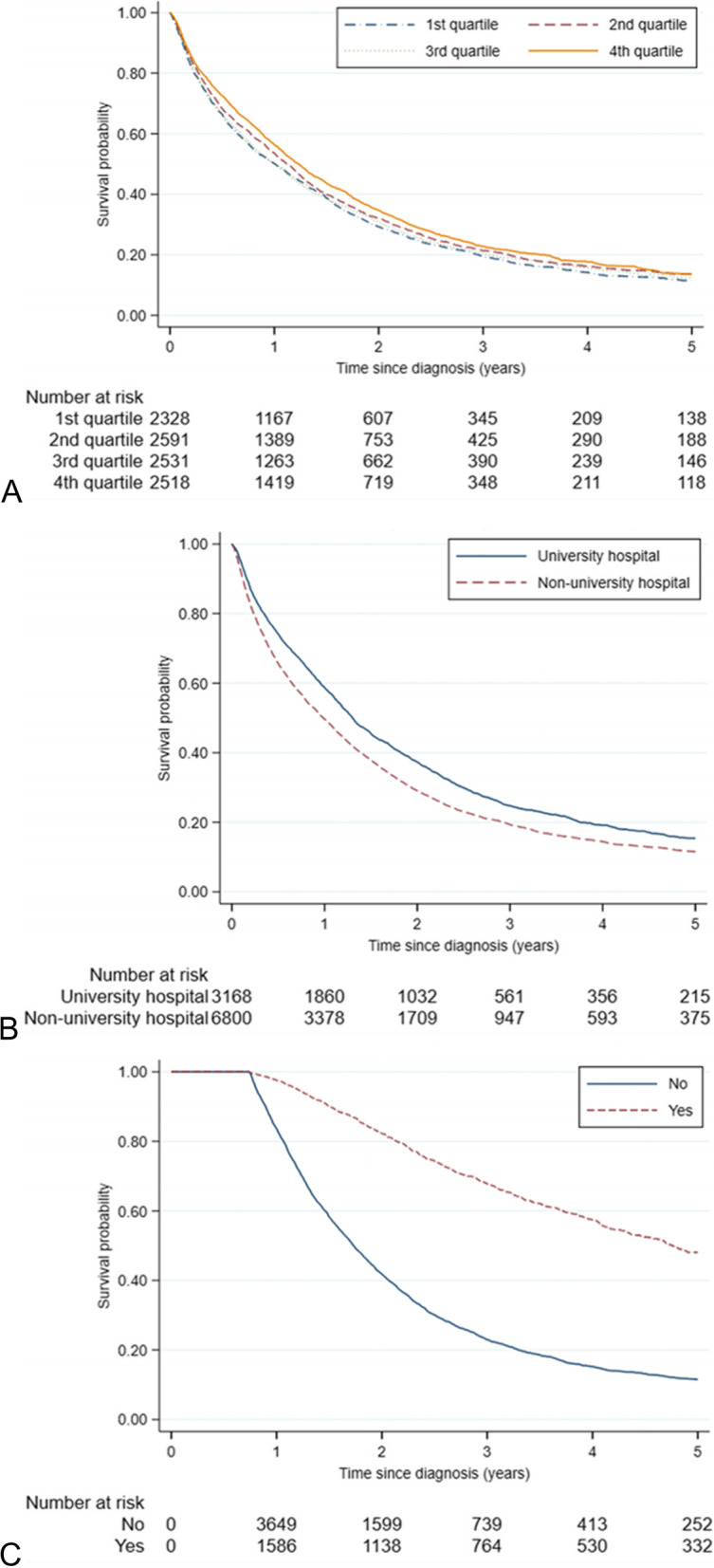
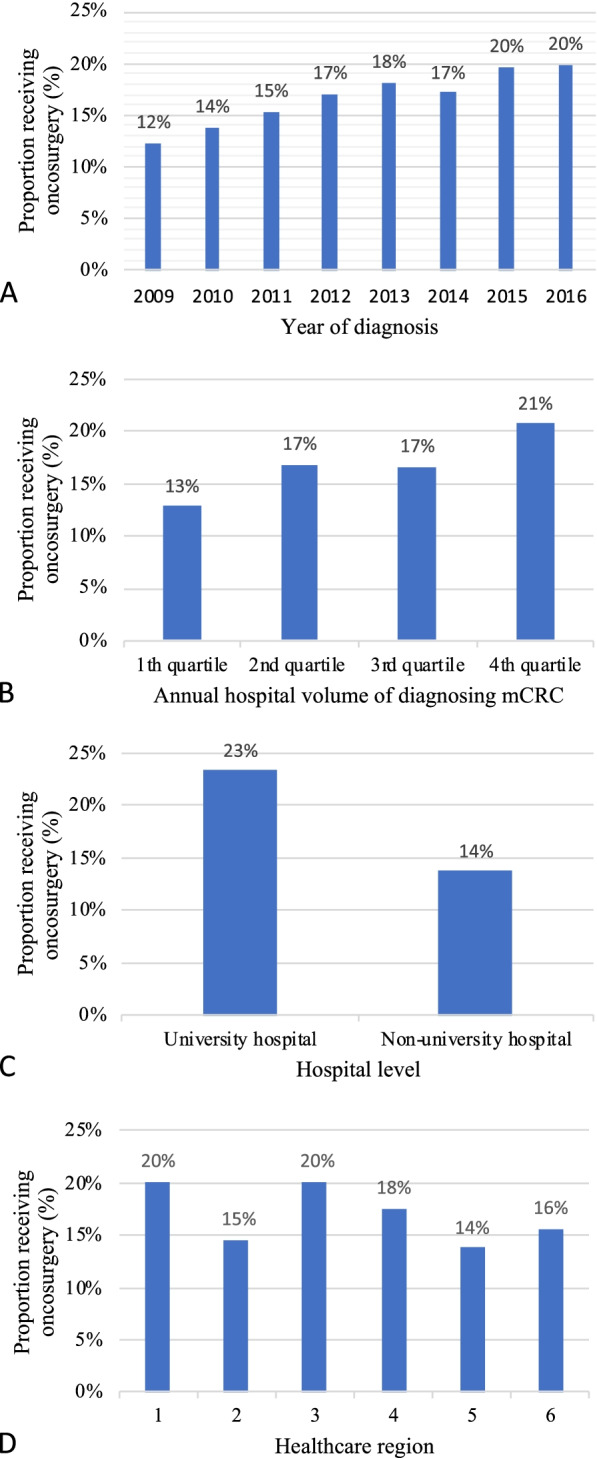
A total of 1,674 (17%) out of 9,968 mCRC patients had metastatic surgery. High hospital volume was not associated with increased odds of metastatic surgery after including hospital level in the model, whereas hospital level was (odds ratio (OR) (95% confidence interval (CI)): 1.94 (1.68-2.24)). All-cause mortality was lower in university versus non-university hospitals (hazard ratio (95% CI): 0.83 (0.78-0.88)).
Patients with mCRC initially cared for by a university hospital experienced a greater chance to receive metastatic surgery and had superior overall survival. High hospital volume in itself was not associated with a greater chance to receive metastatic surgery nor a greater survival probability. Additional efforts should be imposed to provide more equal care for mCRC patients across Swedish hospitals.
仅有有限比例的转移性结直肠癌(mCRC)患者接受转移性手术(包括局部消融治疗)。本研究旨在调查医院容量和医院级别是否与接受转移性手术的机会相关。
本研究从 CRCBaSe 数据库中提取了 2009-2016 年间瑞典所有诊断为同步 mCRC 的成年患者的全国性队列数据。使用逻辑回归和 Cox 回归模型分别评估每年新诊断 mCRC 患者的医院容量与接受转移性手术的机会以及生存之间的关联。以类似的方式评估医院级别(大学/非大学)作为次要暴露。分别拟合单变量和多变量(校正性别、年龄、Charlson 合并症指数、诊断年份、癌症特征和社会经济因素)模型。
在 9968 例 mCRC 患者中,有 1674 例(17%)接受了转移性手术。在纳入医院级别后,高医院容量与接受转移性手术的机会增加无关,而医院级别与接受转移性手术的机会相关(优势比(OR)(95%置信区间(CI)):1.94(1.68-2.24))。与非大学医院相比,大学医院的全因死亡率更低(风险比(95%CI):0.83(0.78-0.88))。
最初在大学医院接受治疗的 mCRC 患者接受转移性手术的机会更大,整体生存率更高。高医院容量本身与接受转移性手术的机会增加或生存率提高无关。应加大力度为瑞典各医院的 mCRC 患者提供更加均等的治疗。