Pediatric Nephrology, Dialysis and Transplant Unit, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Via della Commenda 9, 20122, Milan, Italy.
Laboratory of Regenerative Medicine, Cell Factory, Department of Transfusion Medicine and Hematology, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Via Francesco Sforza 35, 20122, Milan, Italy.
Stem Cell Res Ther. 2022 Aug 19;13(1):420. doi: 10.1186/s13287-022-03112-7.
Children with multi-drug resistant idiopathic nephrotic syndrome (MDR-INS) usually progress to end-stage kidney disease with a consistent risk of disease recurrence after transplantation. New therapeutic options are needed for these patients. Mesenchymal stromal cells (MSCs) are multipotential non-hematopoietic cells with several immunomodulatory properties and growing clinical applications. Cord blood-derived MSC have peculiar anti-inflammatory and immunosuppressive properties. We aimed at assessing safety and efficacy of cord-blood-derived MSCs (CB-MSCs) in children with MDR-INS.
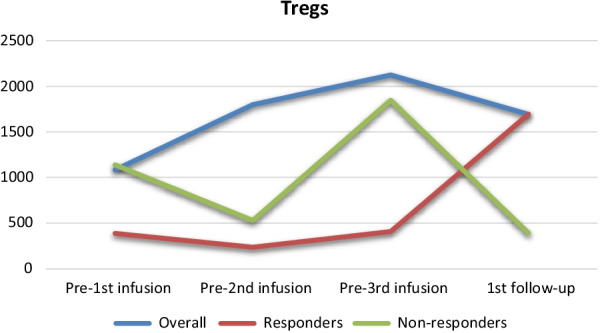
DESIGN, SETTING, PARTICIPANTS: Prospective, open-label, single arm phase I-II pilot study. Pediatric patients with MDR-INS, resistant to at least two lines of therapy, were enrolled. Allogenic CB-MSCs were administered intravenously on days 0, 14, and 21 at a dose of 1.5 × 10 cells/kg. Patients were followed for at least 12 months. The primary outcomes were safety and toxicity. The secondary outcome was remission at 12 months evaluated by urinary protein/urinary creatinine ratio (uPr/uCr). Circulating regulatory T cells (Tregs) were monitored.
Eleven pediatric patients with MDR-INS (10 females, median age 13 years) resistant to a median of 3 previous lines of therapy were enrolled. All patients completed the CB-MSC infusion schedule. No patient experienced any infusion-related adverse event or toxicity. Nine patients were assessable for efficacy. At the 12 months follow-up after the treatment, the median uPr/uCr did not change significantly from baseline (8.13 vs. 9.07; p = 0.98), while 3 patients were in partial or complete remission. A lower baseline uPr/uCr was a predictor of remission (2.55 vs. 8.74; p = 0.0238). Tregs count was not associated with CB-MSCs therapy.
CB-MSCs are safe and may have a role in the immunosuppressive therapy of pediatric patients with MDR-INS. This preliminary experience paves the way toward further phase II studies addressing MSC efficacy in immune-mediated kidney diseases.
患有多重耐药特发性肾病综合征(MDR-INS)的儿童通常会进展为终末期肾病,且在移植后疾病复发的风险持续存在。这些患者需要新的治疗选择。间充质基质细胞(MSCs)是具有多种免疫调节特性且临床应用日益增多的多能非造血细胞。脐血来源的 MSC 具有独特的抗炎和免疫抑制特性。我们旨在评估脐血来源的间充质基质细胞(CB-MSCs)在 MDR-INS 儿童中的安全性和疗效。
设计、地点、参与者:前瞻性、开放标签、单臂 I- II 期试验。招募了患有 MDR-INS 的儿科患者,这些患者对至少两种治疗方案均耐药。在第 0、14 和 21 天,以 1.5×106细胞/kg 的剂量静脉内给予同种异体 CB-MSCs。患者随访至少 12 个月。主要结局是安全性和毒性。次要结局是在 12 个月时通过尿蛋白/尿肌酐比(uPr/uCr)评估的缓解。监测循环调节性 T 细胞(Tregs)。
共纳入 11 例 MDR-INS 患儿(10 例女性,中位年龄 13 岁),对中位 3 线治疗方案耐药。所有患者均完成了 CB-MSC 输注方案。无患者出现任何与输注相关的不良事件或毒性。9 例患者可评估疗效。在治疗后 12 个月的随访中,uPr/uCr 中位数与基线相比无显著变化(8.13 与 9.07;p=0.98),但 3 例患者处于部分缓解或完全缓解。较低的基线 uPr/uCr 是缓解的预测因素(2.55 与 8.74;p=0.0238)。Tregs 计数与 CB-MSCs 治疗无关。
CB-MSCs 是安全的,可能在儿童 MDR-INS 的免疫抑制治疗中发挥作用。这一初步经验为进一步的 MSC 在免疫介导的肾脏疾病中的疗效的 II 期研究铺平了道路。