Boscà-Ramon A, Ratnam L, Cavenagh T, Chun J-Y, Morgan R, Gonsalves M, Das R, Ameli-Renani S, Pavlidis V, Hawthorn B, Ntagiantas N, Mailli L
Department of Radiology, St. George's Hospital, St George's Healthcare NHS Trust, London, SW17 0QT, UK.
CVIR Endovasc. 2022 Aug 20;5(1):43. doi: 10.1186/s42155-022-00315-0.
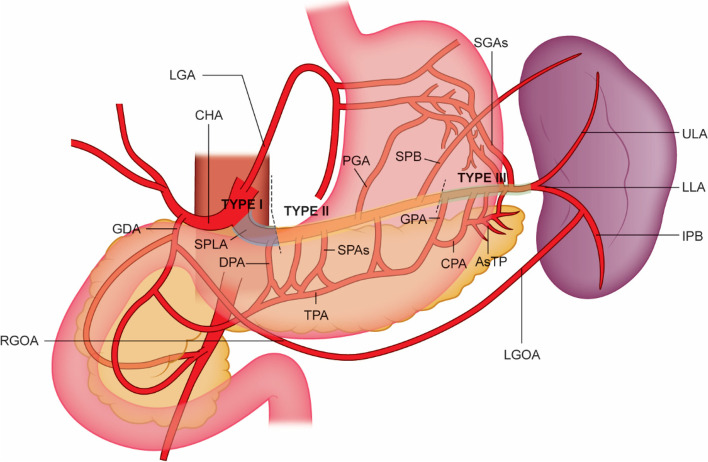
Proximal splenic artery embolisation (PSAE) can be performed in stable patients with Association for the Surgery of Trauma (AAST) grade III-V splenic injury. PSAE reduces splenic perfusion but maintains viability of the spleen and pancreas via the collateral circulation. The hypothesized ideal location is between the dorsal pancreatic artery (DPA) and great pancreatic artery (GPA). This study compares the outcomes resulting from PSAE embolisation in different locations along the splenic artery.
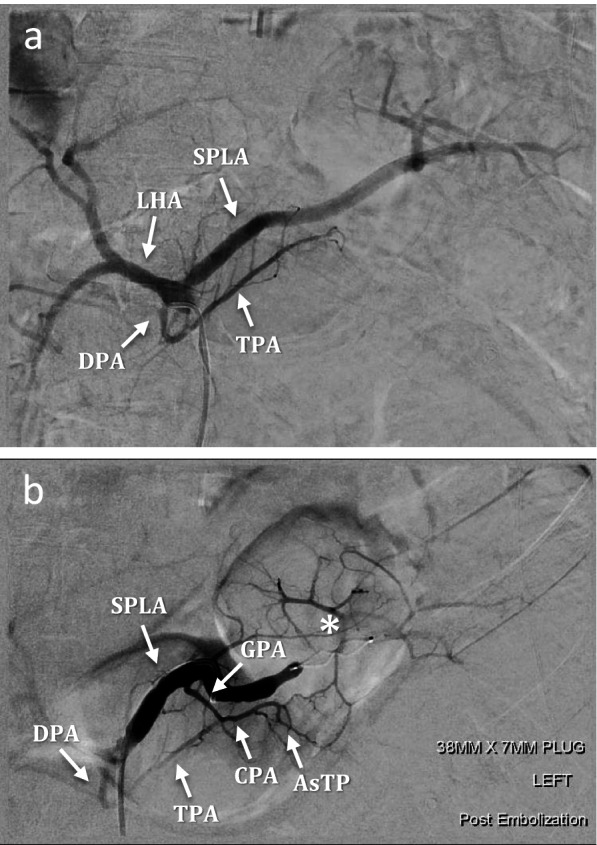
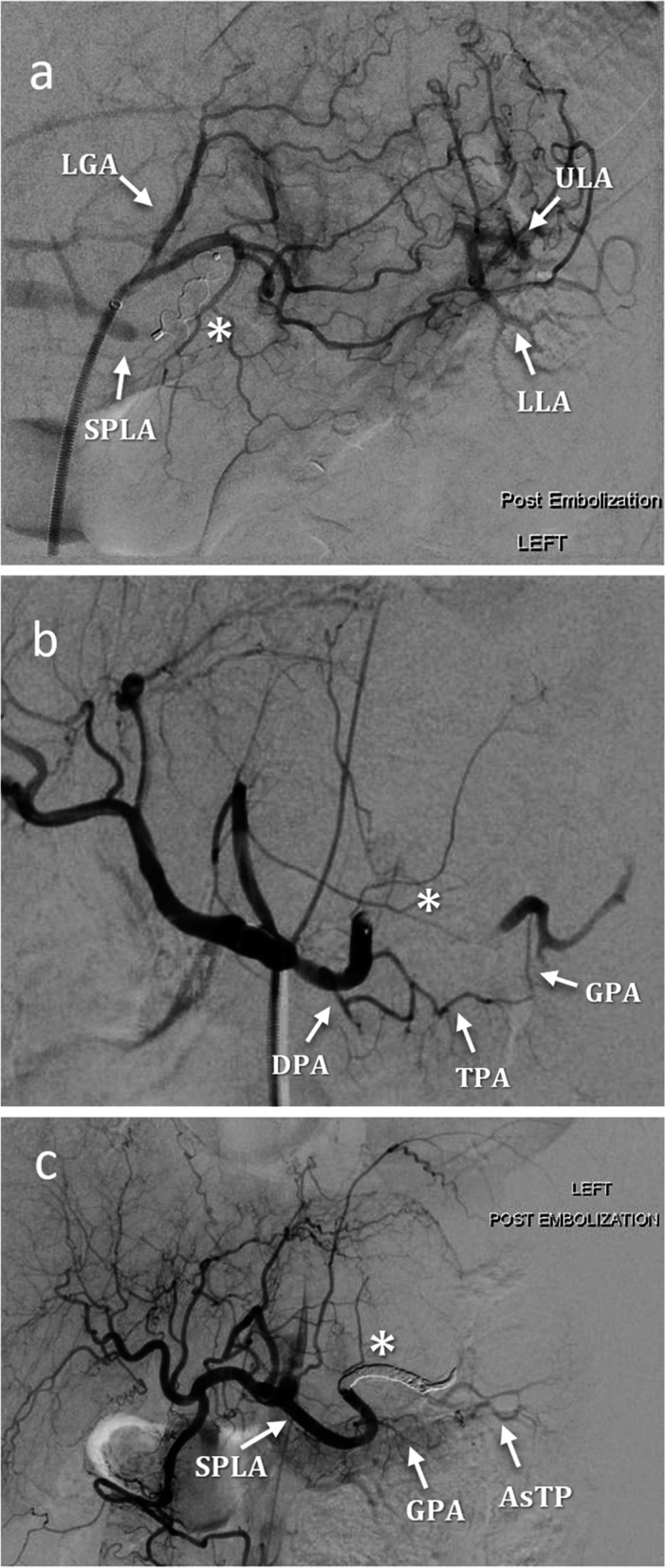
Retrospective review was performed of PSAE for blunt splenic trauma (2015-2020). Embolisation locations were divided into: Type I, proximal to DPA; Type II, DPA-GPA; Type III, distal to GPA. Fifty-eight patients underwent 59 PSAE: Type I (7); Type II (27); Type III (25). Data was collected on technical and clinical success, post-embolisation pancreatitis and splenic perfusion. Statistical significance was assessed using a chi-squared test.
Technical success was achieved in 100% of cases. Clinical success was 100% for Type I/II embolisation and 88% for Type III: one patient underwent reintervention and two had splenectomies for ongoing instability. Clinical success was significantly higher in Type II embolisation compared to Type III (p = 0.02). No episodes of pancreatitis occurred post-embolisation. Where post-procedural imaging was obtained, splenic perfusion remained 100% in Type I and II embolisation and 94% in Type III. Splenic perfusion was significantly higher in the theorized ideal Type II group compared to Type I and III combined (p = 0.01).
The results support the proposed optimal embolisation location as being between the DPA and GPA.
对于创伤外科学会(AAST)分级为III - V级的稳定型脾损伤患者,可进行近端脾动脉栓塞术(PSAE)。PSAE可减少脾脏灌注,但通过侧支循环维持脾脏和胰腺的活力。推测的理想位置在胰背动脉(DPA)和胰大动脉(GPA)之间。本研究比较了沿脾动脉不同位置进行PSAE栓塞的结果。
对2015 - 2020年钝性脾外伤的PSAE进行回顾性研究。栓塞位置分为:I型,DPA近端;II型,DPA - GPA之间;III型,GPA远端。58例患者接受了59次PSAE:I型(7例);II型(27例);III型(25例)。收集了技术和临床成功率、栓塞后胰腺炎及脾脏灌注的数据。使用卡方检验评估统计学意义。
所有病例技术成功率均为100%。I/II型栓塞的临床成功率为100%,III型为88%:1例患者接受了再次干预,2例因持续不稳定接受了脾切除术。II型栓塞的临床成功率显著高于III型(p = 0.02)。栓塞后未发生胰腺炎。在获得术后影像学检查的病例中,I型和II型栓塞的脾脏灌注保持100%,III型为94%。理论上理想的II型组的脾脏灌注显著高于I型和III型联合组(p = 0.01)。
结果支持提议的最佳栓塞位置在DPA和GPA之间。