Hospital for Sick Children, Toronto, Ontario, Canada.
Cundill Centre for Child and Youth Depression, Centre for Addiction and Mental Health, Toronto, Ontario, Canada.
JAMA Netw Open. 2022 Aug 1;5(8):e2227119. doi: 10.1001/jamanetworkopen.2022.27119.
Understanding the longitudinal, bidirectional associations between disturbed sleep and depression in childhood and adolescence is crucial for the development of prevention and intervention programs.
To test for bidirectional associations and cascade processes between disturbed sleep and depressive symptoms covering both childhood and adolescence and to test for the moderating processes of sex and pubertal status in adolescence.
DESIGN, SETTING, AND PARTICIPANTS: A prospective cohort study using the Québec Longitudinal Study of Child Development (QLSCD; 1997-ongoing). QLSCD's objective is to identify early childhood factors associated with long-term psychosocial and academic adjustment. Data were collected across 8 waves between ages 5 years (2003) and 17 years (2015). Associations were tested through cross-lagged models in childhood (5, 7, and 8 years), and in adolescence (10, 12, 13, 15, and 17 years). Data were analyzed from February to October 2021.
Primary outcomes were disturbed sleep and depressive symptoms. Disturbed sleep was parent-reported and included sleep duration, time awake in bed, daytime sleepiness, sleep talking, sleepwalking, night terrors, and nightmares. Depressive symptoms were parent-reported in childhood (Child Behavior Checklist and Revised Ontario Child Health Study Scales), and self-reported in adolescence (Mental Health and Social Inadaptation Assessment for Adolescents).
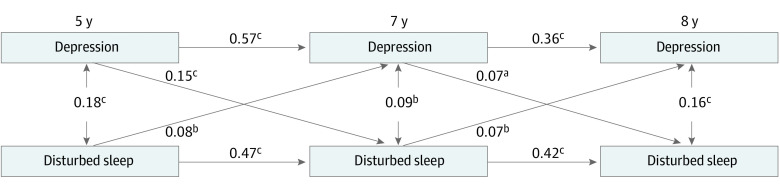
Data on 1689 children (852 female [50.4%]) and 1113 adolescents (595 female [53.5%]) were included in the analyses. In childhood, significant bidirectional associations between depressive symptoms and disturbed sleep at all time points were found, indicating cascade processes (range β = 0.07; 95% CI, 0.02-012 to β = 0.15; 95% CI, 0.10-0.19). In adolescence, significant bidirectional associations from depressive symptoms to disturbed sleep (β = 0.09; 95% CI, 0.04-0.14) and vice versa (β = 0.10; 95% CI, 0.04-0.16) between 10 and 12 years were found. Between 12 and 13 years, depressive symptoms were modestly associated with disturbed sleep (β = 0.05; 95% CI, 0.001-0.10) but the reverse association was not significant. Cross-lagged estimates were nonsignificant after 13 years. The associations did not vary as a function of either sex or puberty-by-sex.
These findings suggest that disturbed sleep is associated with the consolidation of depressive symptoms starting in childhood, which, in turn, is associated with ongoing sleep problems. It is possible that timely and appropriate interventions for incipient disturbed sleep and depression prevent spiraling effects on both domains.
了解儿童期和青春期睡眠障碍与抑郁之间的纵向、双向关联对于制定预防和干预计划至关重要。
测试睡眠障碍和抑郁症状在儿童期和青春期的双向关联和级联过程,并测试性别和青春期状态在青春期的调节作用。
设计、地点和参与者:这是一项使用魁北克儿童发展纵向研究(QLSCD;1997 年至今)的前瞻性队列研究。QLSCD 的目的是确定与长期心理社会和学业适应相关的早期儿童因素。数据通过 8 个波次收集,年龄范围在 5 岁(2003 年)至 17 岁(2015 年)之间。通过儿童期(5、7 和 8 岁)和青春期(10、12、13、15 和 17 岁)的交叉滞后模型测试关联。数据于 2021 年 2 月至 10 月进行分析。
主要结果是睡眠障碍和抑郁症状。睡眠障碍由家长报告,包括睡眠时间、卧床时间、日间嗜睡、说梦话、梦游、夜惊和噩梦。儿童期的抑郁症状由家长报告(儿童行为检查表和修订后的安大略省儿童健康研究量表),青春期由自我报告(青少年心理健康和社会适应评估)。
分析纳入了 1689 名儿童(852 名女性[50.4%])和 1113 名青少年(595 名女性[53.5%])的数据。在儿童期,发现所有时间点抑郁症状和睡眠障碍之间存在显著的双向关联,表明存在级联过程(范围β=0.07;95%CI,0.02-0.12 至β=0.15;95%CI,0.10-0.19)。在青春期,发现抑郁症状与睡眠障碍之间存在显著的双向关联(β=0.09;95%CI,0.04-0.14)和反之亦然(β=0.10;95%CI,0.04-0.16)在 10 到 12 岁之间。在 12 至 13 岁之间,抑郁症状与睡眠障碍适度相关(β=0.05;95%CI,0.001-0.10),但反向关联不显著。13 岁后,交叉滞后估计值无统计学意义。这些关联不受性别或青春期性别影响。
这些发现表明,睡眠障碍与儿童期开始的抑郁症状巩固有关,而抑郁症状又与持续的睡眠问题有关。及时和适当的针对初期睡眠障碍和抑郁的干预措施可能会防止这两个领域的螺旋式下降效应。