Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, Canada.
Department of Medicine, McMaster University, HSC 3V38, 1280 Main Street West, Hamilton, ON, L8S 4K1, Canada.
Cardiovasc Diabetol. 2022 Aug 22;21(1):158. doi: 10.1186/s12933-022-01594-6.
The estimated glomerular filtration rate (eGFR) and the albumin-to-creatinine ratio (ACR) are risk factors for diabetes-related outcomes. A composite that captures information from both may provide a simpler way of assessing risk.
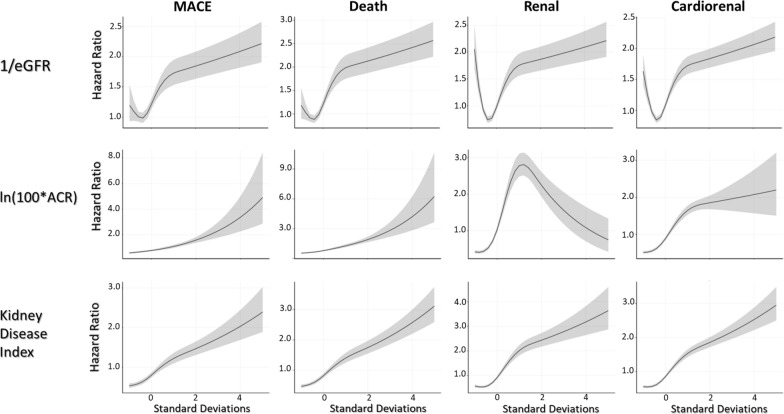
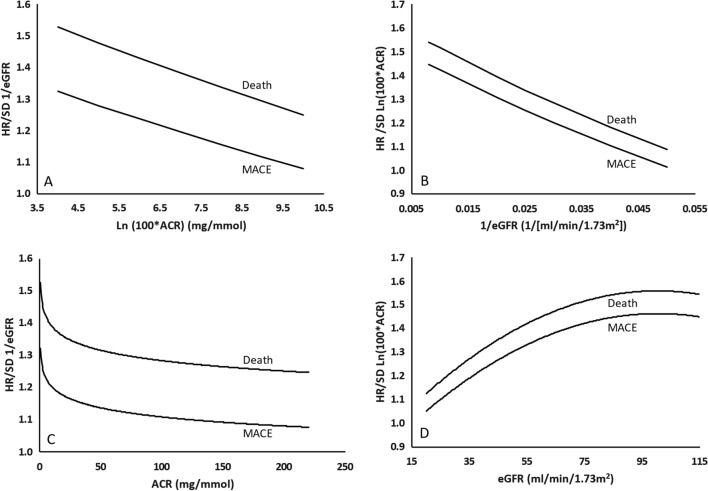
9115 of 9901 Researching Cardiovascular Events with a Weekly Incretin in Diabetes (REWIND) participants with both an ACR and eGFR at baseline were included in this post hoc epidemiologic analysis. The hazard of higher baseline levels of 1/eGFR and natural log transformed ACR (calculated as ln [ACR × 100] to eliminate negative values) and their interaction for incident major adverse cardiovascular events (MACE), kidney outcomes, and deaths was estimated. The hazard of the geometric mean of these two baseline measures (the kidney disease index or KDI) was also assessed.
A non-linear relationship was observed between 1/eGFR and all three outcomes, and between ln [ACR × 100] and the kidney outcome. There was also a negative interaction between these two risk factors with respect to MACE and death. Conversely, a linear relationship was noted between the KDI and all three outcomes. People in the highest KDI fifth experienced the highest incidence of MACE, death, and the kidney outcome (4.43, 4.56, and 5.55/100 person-years respectively). C statistics for the KDI were similar to those for eGFR and albuminuria.
The KDI combines the baseline eGFR and ACR into a novel composite risk factor that has a simple linear relationship with incident serious outcomes in people with diabetes and additional CV risk factors. Trial Registration clinicaltrials.gov NCT01394952.
估算肾小球滤过率(eGFR)和白蛋白与肌酐比值(ACR)是与糖尿病相关结局的风险因素。综合这两个因素的信息可能提供一种更简单的评估风险的方法。
在研究心血管事件与每周使用肠降血糖素治疗糖尿病(REWIND)研究中,共纳入 9901 例患者中的 9115 例基线时同时具有 ACR 和 eGFR 的患者。采用事后流行病学分析,评估基线时更高水平的 1/eGFR 和自然对数转换的 ACR(ln [ACR × 100],以消除负值)及其交互作用对于发生主要不良心血管事件(MACE)、肾脏结局和死亡的风险。还评估了这两个基线测量值(肾脏病指数或 KDI)的几何平均值的风险。
观察到 1/eGFR 与所有三种结局以及 ln [ACR × 100]与肾脏结局之间存在非线性关系。这两个危险因素之间也存在 MACE 和死亡的负交互作用。相反,KDI 与所有三种结局之间呈线性关系。KDI 最高的第 5 五分位数的人发生 MACE、死亡和肾脏结局的风险最高(分别为 4.43、4.56 和 5.55/100 人年)。KDI 的 C 统计值与 eGFR 和白蛋白尿相似。
KDI 将基线 eGFR 和 ACR 组合成一个新的复合风险因素,与糖尿病和其他心血管危险因素患者的严重结局具有简单的线性关系。
clinicaltrials.gov NCT01394952。