Tran Zachary, Hadaya Joseph, Downey Peter, Sanaiha Yas, Verma Arjun, Shemin Richard J, Benharash Peyman
Division of Cardiac Surgery, Department of Surgery, Cardiovascular Outcomes Research Laboratories (CORELAB), David Geffen School of Medicine at UCLA, Los Angeles, Calif.
Department of Cardiovascular and Thoracic Surgery, University of Kansas Health System, Kansas City, Kan.
JTCVS Open. 2022 Feb 24;10:148-161. doi: 10.1016/j.xjon.2022.02.019. eCollection 2022 Jun.
Although patients with significant coronary artery disease and aortic stenosis have traditionally undergone open valve replacement and bypass grafting, percutaneous coronary intervention (PCI) and transcatheter aortic valve replacement (TAVR) are increasingly considered. Because of the lack of data regarding timing of PCI/TAVR, in the present study we evaluated associations of staged and concomitant PCI/TAVR on outcomes in a nationally representative cohort.
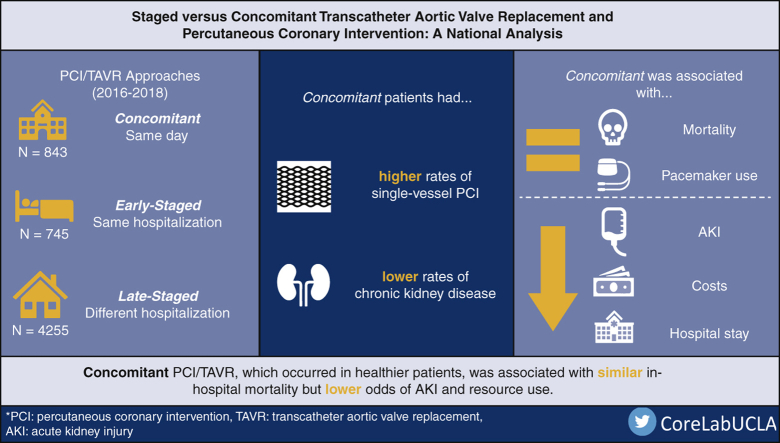
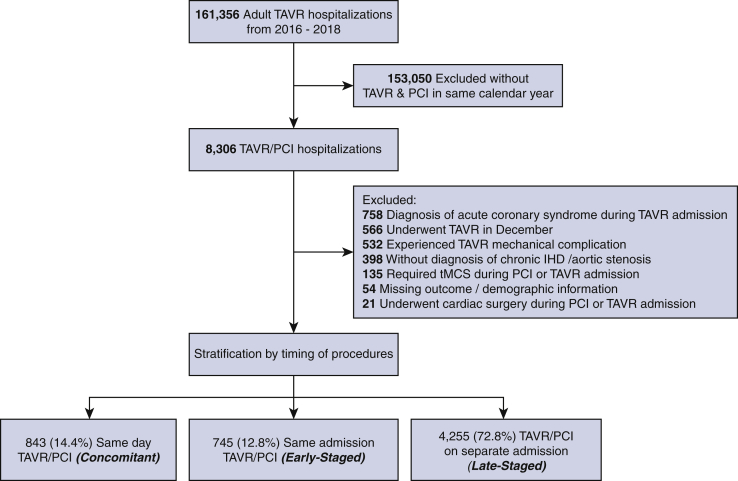
Adults who underwent TAVR and PCI were identified using the 2016 to 2018 Nationwide Readmissions Database. If PCI/TAVR occurred on the same day, patients were considered Concomitant and otherwise considered Staged. Staged were further classified as Early-Staged if both occurred in the same hospitalization or Late-Staged if TAVR ensued PCI in a subsequent hospitalization. Multivariable regression models were developed to evaluate the association of TAVR timing on outcomes. The primary end point was in-hospital mortality whereas perioperative complications including acute kidney injury and hospitalization costs were secondarily considered.
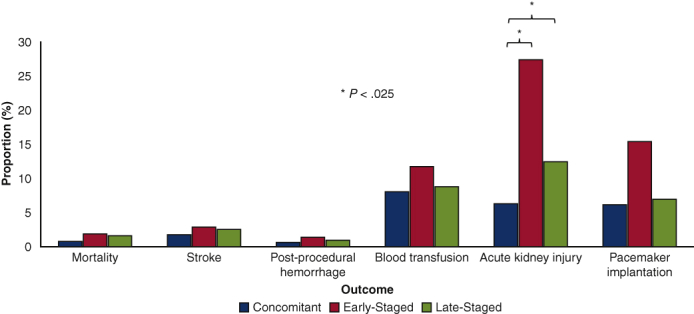
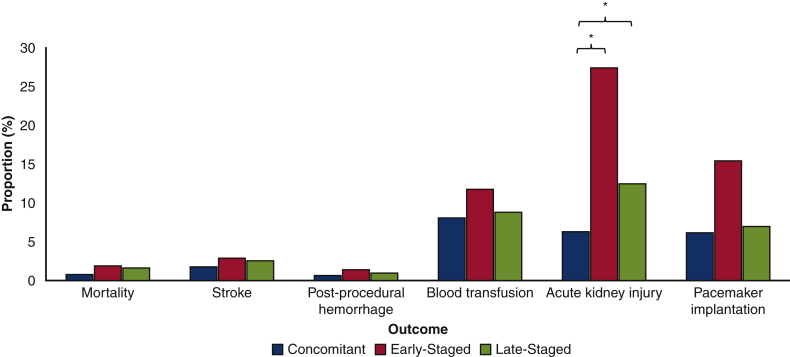
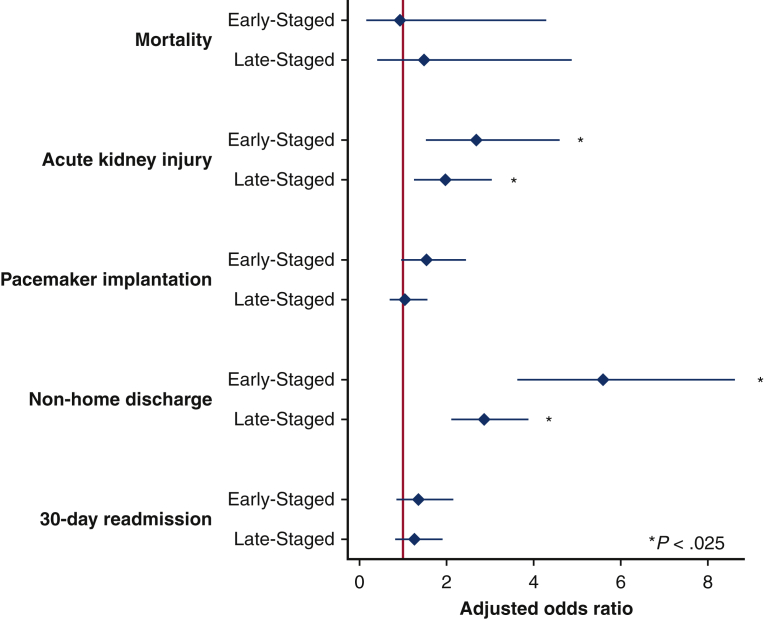
Of an estimated 5843 patients, 843 (14.4%) were Concomitant and 745 (12.7%) and 4255 (72.8%) were Early-Staged and Late-Staged, respectively. Although age and TAVR access were similar, Concomitant had a lower proportion of chronic kidney disease and more commonly underwent single-vessel PCI. Staged showed similar risk-adjusted mortality but greater odds of acute kidney injury (Early-Staged adjusted odds ratio: 2.68; 95% CI, 1.57-4.55 and Late-Staged: 1.97; 95% CI, 1.29-2.99) compared with Concomitant. Although post-TAVR hospitalization duration was similar, total length of stay and costs were increased in Staged.
Concomitant PCI/TAVR was associated with similar rates of in-hospital mortality but reduced rates of acute kidney injury and lower resource utilization. While evaluating patient-specific factors, concomitant PCI/TAVR might be reasonable in select individuals.
尽管患有严重冠状动脉疾病和主动脉瓣狭窄的患者传统上会接受开胸瓣膜置换术和冠状动脉搭桥术,但经皮冠状动脉介入治疗(PCI)和经导管主动脉瓣置换术(TAVR)越来越受到关注。由于缺乏关于PCI/TAVR时机的数据,在本研究中,我们在一个具有全国代表性的队列中评估了分期和同期PCI/TAVR与预后的相关性。
使用2016年至2018年全国再入院数据库识别接受TAVR和PCI的成年人。如果PCI/TAVR在同一天进行,患者被视为同期,否则被视为分期。如果两者在同一住院期间发生,分期患者进一步分为早期分期;如果TAVR在随后的住院期间在PCI之后进行,则分为晚期分期。建立多变量回归模型以评估TAVR时机与预后的相关性。主要终点是住院死亡率,而围手术期并发症包括急性肾损伤和住院费用则作为次要考虑因素。
在估计的5843例患者中,843例(14.4%)为同期,745例(12.7%)和4255例(72.8%)分别为早期分期和晚期分期。尽管年龄和TAVR入路相似,但同期患者的慢性肾病比例较低,且更常接受单支血管PCI。与同期相比,分期患者的风险调整死亡率相似,但急性肾损伤的几率更高(早期分期调整优势比:2.68;95%CI,1.57 - 4.55;晚期分期:1.97;95%CI,1.29 - 2.99)。尽管TAVR后住院时间相似,但分期患者的总住院时间和费用增加。
同期PCI/TAVR与住院死亡率相似,但急性肾损伤发生率降低且资源利用较少。在评估患者个体因素时,对于特定个体,同期PCI/TAVR可能是合理的。