Department of Radiation Oncology, University of California, Los Angeles, California.
Department of Radiation Oncology, Cedars-Sinai Medical Center, Los Angeles, California.
Int J Radiat Oncol Biol Phys. 2023 Jan 1;115(1):142-152. doi: 10.1016/j.ijrobp.2022.08.041. Epub 2022 Aug 23.
Postoperative radiation therapy (RT) is an underused standard-of-care intervention for patients with prostate cancer and recurrence/adverse pathologic features after radical prostatectomy. Although stereotactic body RT (SBRT) is a well-studied and convenient option for definitive treatment, data on the postprostatectomy setting are extremely limited. The purpose of this study was to evaluate short-term physician-scored genitourinary (GU) and gastrointestinal (GI) toxicities and patient-reported outcomes after postprostatectomy SBRT.
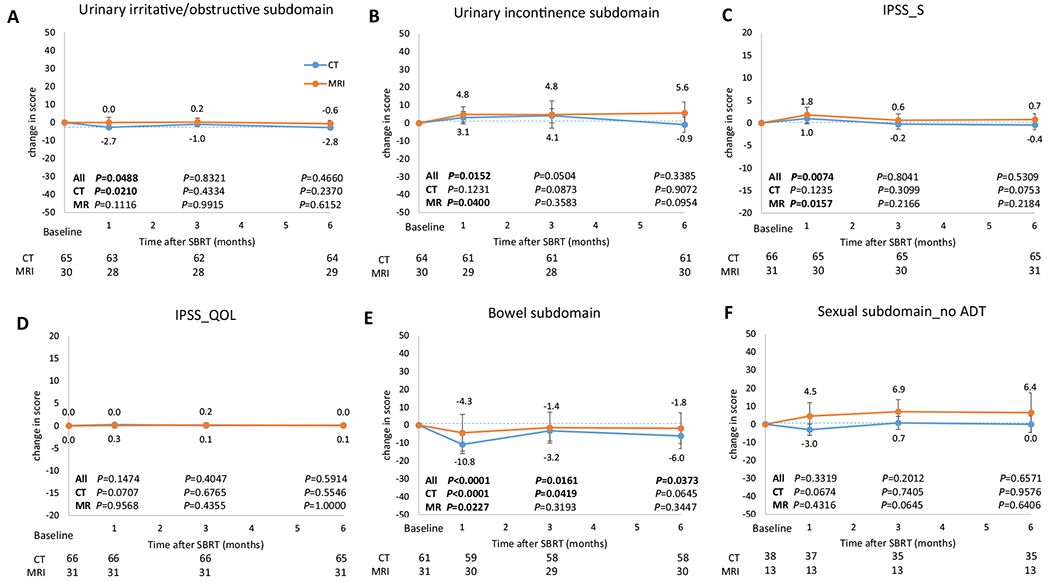
The SCIMITAR trial was a phase 2, dual-center, open-label, single-arm trial that enrolled patients with postoperative prostate-specific antigen >0.03 ng/mL or adverse pathologic features. Coprimary endpoints were 4-year biochemical recurrence-free survival, physician-scored acute and late GU and GI toxicities by the Common Terminology Criteria for Adverse Events (version 4.03) scale, and patient-reported quality-of-life (QOL) outcomes, as represented by the Expanded Prostate Cancer Index-26 and the International Prostate Symptom Score. Patients received SBRT 30 to 34 Gy/5 fractions to the prostate bed ± bed boost ± pelvic nodes with computed tomography (CTgRT) or magnetic resonance imaging guidance (MRgRT) in a nonrandomized fashion. Physician-scored toxicities and patient-reported QOL outcomes were collected at baseline and at 1, 3, and 6 months of follow-up. Univariable and multivariable analyses were performed to evaluate predictors of toxicities and QOL outcomes.
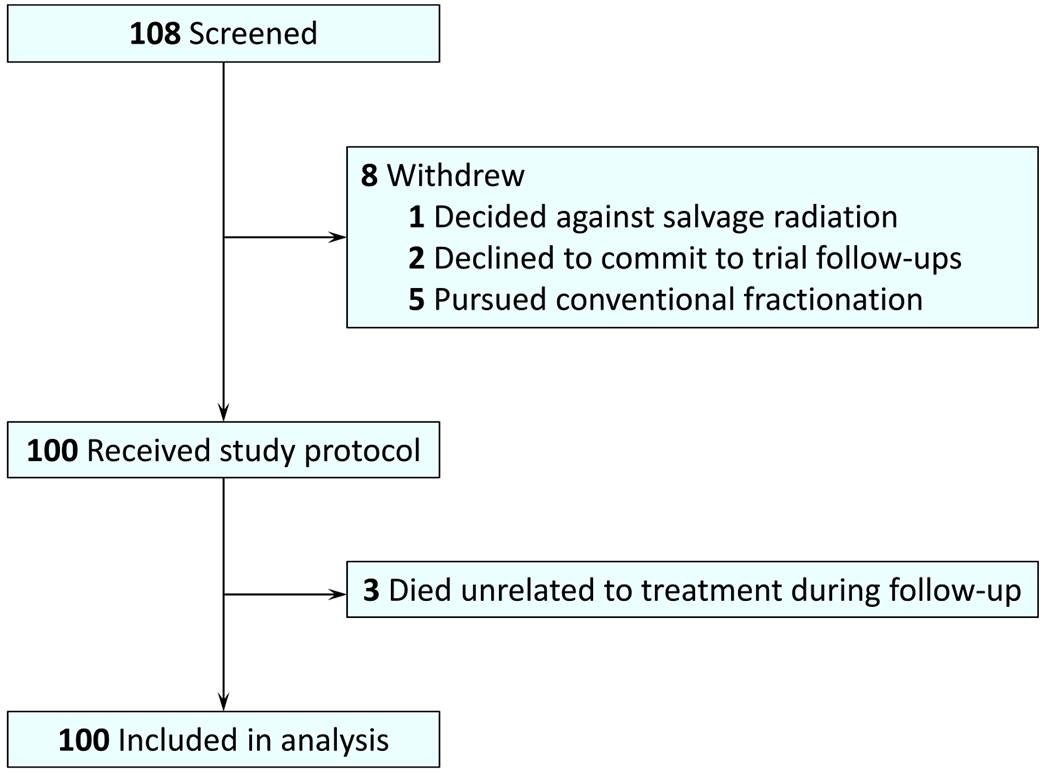
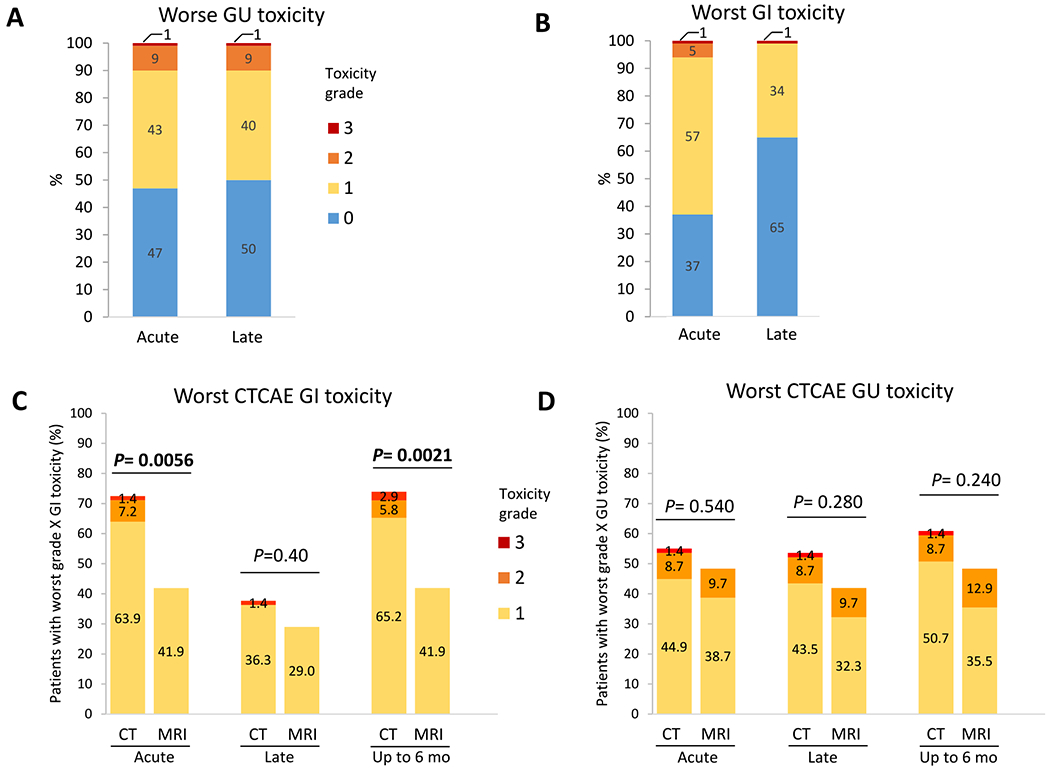
One hundred participants were enrolled (CTgRT, n = 69; MRgRT, n = 31). The median follow-up was 29.5 months (CTgRT: 33.3 months, MRgRT: 22.6 months). The median (range) prostate bed dose was 32 (30-34) Gy. Acute and late grade 2 GU toxicities were both 9% while acute and late grade 2 GI toxicities were 5% and 0%, respectively. Three patients had grade 3 toxicity (n = 1 GU, n = 2 GI). No patient receiving MRgRT had grade 3 GU or grade ≥2 GI toxicity. Compared with CTgRT, MRgRT was associated with a 30.5% (95% confidence interval, 11.6%-49.5%) reduction in any-grade acute GI toxicity (P = .006). MRgRT was independently associated with improved any-grade GI toxicity and improved bowel QOL.
Postprostatectomy SBRT was well tolerated at short-term follow-up. MRgRT may decrease GI toxicity. Longer toxicity and/or efficacy follow-up and randomized studies are needed.
术后放疗(RT)是前列腺癌患者根治性前列腺切除术后复发/不良病理特征的标准治疗方法,但应用不足。立体定向体部放疗(SBRT)是一种已充分研究且方便的确定性治疗选择,但在前列腺切除术后的应用数据极为有限。本研究旨在评估前列腺切除术后 SBRT 后短期医生评分的泌尿生殖系统(GU)和胃肠道(GI)毒性和患者报告的结局。
SCIMITAR 试验是一项 2 期、双中心、开放标签、单臂试验,招募了前列腺特异性抗原(PSA)>0.03ng/ml 或有不良病理特征的术后患者。主要终点是 4 年生化无复发生存率、医生根据不良事件通用术语标准(第 4.03 版)评分的急性和晚期 GU 和 GI 毒性,以及患者报告的生活质量(QOL)结局,代表扩展前列腺癌指数-26 和国际前列腺症状评分。患者采用 CTgRT 或 MRgRT 以 30 至 34Gy/5 个剂量照射前列腺床±床增量±盆腔淋巴结,以非随机方式进行。医生评分的毒性和患者报告的 QOL 结局在基线以及随访 1、3 和 6 个月时收集。进行单变量和多变量分析以评估毒性和 QOL 结局的预测因素。
共纳入 100 名参与者(CTgRT,n=69;MRgRT,n=31)。中位随访时间为 29.5 个月(CTgRT:33.3 个月,MRgRT:22.6 个月)。中位(范围)前列腺床剂量为 32(30-34)Gy。急性和晚期 2 级 GU 毒性均为 9%,而急性和晚期 2 级 GI 毒性分别为 5%和 0%。3 名患者出现 3 级毒性(GU 1 级,GI 2 级)。接受 MRgRT 的患者无 3 级 GU 或≥2 级 GI 毒性。与 CTgRT 相比,MRgRT 使任何级别急性 GI 毒性降低 30.5%(95%置信区间,11.6%-49.5%;P=0.006)。MRgRT 与改善的任何级别 GI 毒性和改善的肠道 QOL 相关。
前列腺切除术后 SBRT 在短期随访中耐受性良好。MRgRT 可能降低 GI 毒性。需要进行更长时间的毒性和/或疗效随访和随机研究。