Department of Radiation Oncology, University of California Los Angeles, 200 Medical Plaza Driveway, Suite # B265, Medical Plaza Driveway, Los Angeles, CA, 90095, USA.
Department of Medicine Statistics Core, University of California Los Angeles, 200 Medical Plaza Driveway, Suite # B265, Medical Plaza Driveway, Los Angeles, CA, 90095, USA.
BMC Cancer. 2021 May 11;21(1):538. doi: 10.1186/s12885-021-08281-x.
Stereotactic body radiotherapy (SBRT) is becoming increasingly used in treating localized prostate cancer (PCa), with evidence showing similar toxicity and efficacy profiles when compared with longer courses of definitive radiation. Magnetic resonance imaging (MRI)-guided radiotherapy has multiple potential advantages over standard computed tomography (CT)-guided radiotherapy, including enhanced prostate visualization (abrogating the need for fiducials and MRI fusion), enhanced identification of the urethra, the ability to track the prostate in real-time, and the capacity to perform online adaptive planning. However, it is unknown whether these potential advantages translate into improved outcomes. This phase III randomized superiority trial is designed to prospectively evaluate whether toxicity is lower after MRI-guided versus CT-guided SBRT.
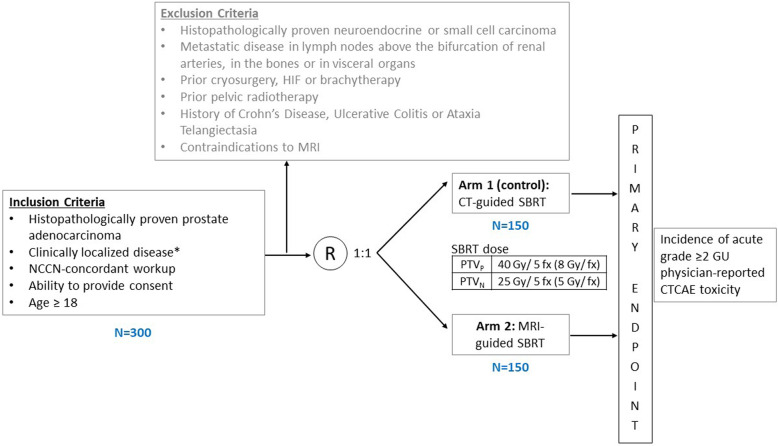
Three hundred men with localized PCa will be randomized in a 1:1 ratio to SBRT using CT or MRI guidance. Randomization will be stratified by baseline International Prostate Symptom Score (IPSS) (≤15 or > 15) and prostate gland volume (≤50 cc or > 50 cc). Five fractions of 8 Gy will be delivered to the prostate over the course of fourteen days, with or without hormonal therapy and elective nodal radiotherapy (to a dose of 5 Gy per fraction) as per the investigator's discretion. The primary endpoint is the incidence of physician-reported acute grade ≥ 2 genitourinary (GU) toxicity (during the first 90 days after SBRT), as assessed by the CTCAE version 4.03 scale. Secondary clinical endpoints include incidence of acute grade ≥ 2 gastrointestinal (GI) toxicity, 5-year cumulative incidences of physician-reported late grade ≥ 2 GU and GI toxicity, temporal changes in patient-reported quality of life (QOL) outcomes, 5-year biochemical recurrence-free survival and the proportion of fractions of MRI-guided SBRT in which online adaptive radiotherapy is used.
The MIRAGE trial is the first randomized trial comparing MRI-guided with standard CT-guided SBRT for localized PCa. The primary hypothesis is that MRI-guided SBRT will lead to an improvement in the cumulative incidence of acute grade ≥ 2 GU toxicity when compared to CT-guided SBRT. The pragmatic superiority design focused on an acute toxicity endpoint will allow an early comparison of the two technologies.
Clinicaltrials.gov identifier: NCT04384770. Date of registration: May 12, 2020. https://clinicaltrials.gov/ct2/show/NCT04384770 PROTOCOL VERSION: Version 2.1, Aug 28, 2020.
立体定向体放射治疗(SBRT)在治疗局限性前列腺癌(PCa)中的应用越来越广泛,其与标准的根治性放疗相比,具有相似的毒性和疗效。与标准的计算机断层扫描(CT)引导放疗相比,磁共振成像(MRI)引导放疗具有多种潜在优势,包括增强前列腺的可视化(消除了对基准和 MRI 融合的需求)、增强对尿道的识别、实时跟踪前列腺的能力,以及进行在线自适应计划的能力。然而,目前尚不清楚这些潜在的优势是否会转化为改善结果。本项 III 期随机优势试验旨在前瞻性评估 MRI 引导与 CT 引导 SBRT 后毒性是否更低。
300 名局限性 PCa 患者将以 1:1 的比例随机分为 SBRT 使用 CT 或 MRI 引导组。随机化将按基线国际前列腺症状评分(IPSS)(≤15 或>15)和前列腺体积(≤50cc 或>50cc)进行分层。在 14 天内给予前列腺 5 次 8Gy 的剂量,是否联合激素治疗和选择性淋巴结放疗(每次 5Gy)由研究者决定。主要终点是研究者报告的急性 2 级及以上泌尿生殖系统(GU)毒性的发生率(SBRT 后 90 天内),采用 CTCAE 第 4.03 版量表评估。次要临床终点包括急性 2 级及以上胃肠道(GI)毒性的发生率、5 年累积发生率、患者报告的晚期 2 级及以上 GU 和 GI 毒性、患者报告的生存质量(QOL)结局的时间变化、5 年生化无复发生存率以及 MRI 引导 SBRT 中在线自适应放疗使用的比例。
MIRAGE 试验是比较局部前列腺癌 MRI 引导与标准 CT 引导 SBRT 的首个随机试验。主要假设是与 CT 引导 SBRT 相比,MRI 引导 SBRT 可降低急性 2 级及以上 GU 毒性的累积发生率。重点关注急性毒性终点的实用优势设计将允许对两种技术进行早期比较。
Clinicaltrials.gov 标识符:NCT04384770。注册日期:2020 年 5 月 12 日。https://clinicaltrials.gov/ct2/show/NCT04384770 方案版本:第 2.1 版,2020 年 8 月 28 日。