UOC Resuscitation, Intensive and Sub-Intensive Care, National Institute for Infectious Diseases IRCCS Lazzaro Spallanzani, 00149 Rome, Italy.
Department of Epidemiology, National Institute for Infectious Diseases IRCCS Lazzaro Spallanzani, 00149 Rome, Italy.
Medicina (Kaunas). 2022 Aug 15;58(8):1104. doi: 10.3390/medicina58081104.
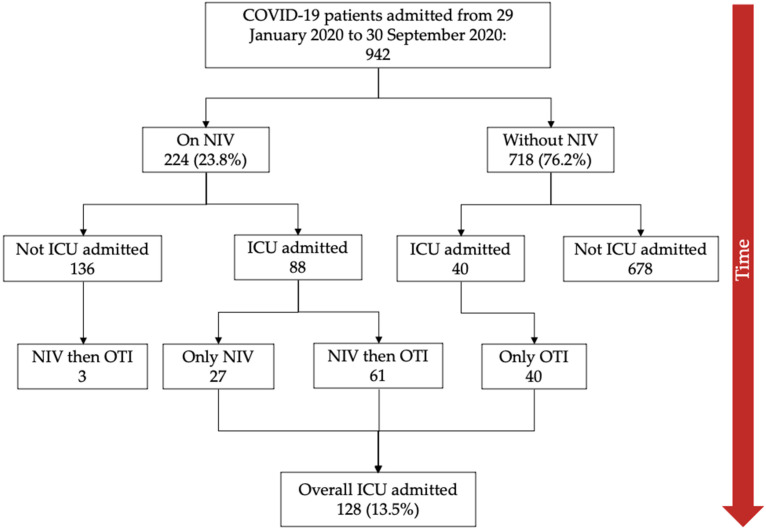
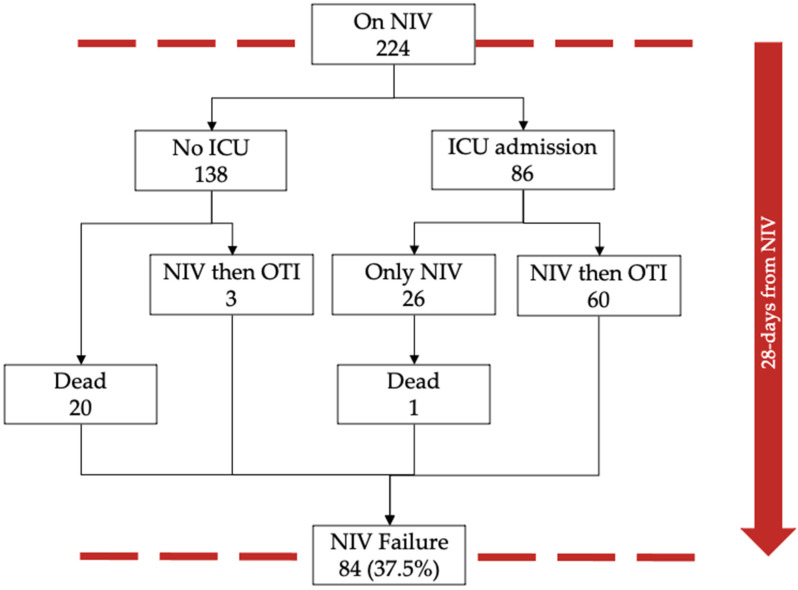
Background and Objectives: Background: Coronavirus disease 2019 (COVID-19) is a novel cause of Acute Respiratory Distress Syndrome (ARDS). Noninvasive ventilation (NIV) is widely used in patients with ARDS across several etiologies. Indeed, with the increase of ARDS cases due to the COVID-19 pandemic, its use has grown significantly in hospital wards. However, there is a lack of evidence to support the efficacy of NIV in patients with COVID-19 ARDS. Materials and Methods: We conducted an observational cohort study including adult ARDS COVID-19 patients admitted in a third level COVID-center in Rome, Italy. The study analyzed the rate of NIV failure defined by the occurrence of orotracheal intubation and/or death within 28 days from starting NIV, its effectiveness, and the associated relative risk of death. The factors associated with the outcomes were identified through logistic regression analysis. Results: During the study period, a total of 942 COVID-19 patients were admitted to our hospital, of which 307 (32.5%) presented with ARDS at hospitalization. During hospitalization 224 (23.8%) were treated with NIV. NIV failure occurred in 84 (37.5%) patients. At 28 days from starting NIV, moderate and severe ARDS had five-fold and twenty-fold independent increased risk of NIV failure (adjusted odds ratio, aOR = 5.01, 95% CI 2.08−12.09, and 19.95, 95% CI 5.31−74.94), respectively, compared to patients with mild ARDS. A total of 128 patients (13.5%) were admitted to the Intensive Care Unit (ICU). At 28-day from ICU admission, intubated COVID-19 patients treated with early NIV had 40% lower mortality (aOR 0.60, 95% CI 0.25−1.46, p = 0.010) compared with patients that underwent orotracheal intubation without prior NIV. Conclusions: These findings show that NIV failure was independently correlated with the severity category of COVID-19 ARDS. The start of NIV in COVID-19 patients with mild ARDS (P/F > 200 mmHg) appears to increase NIV effectiveness and reduce the risk of orotracheal intubation and/or death. Moreover, early NIV (P/F > 200 mmHg) treatment seems to reduce the risk of ICU mortality at 28 days from ICU admission.
背景:2019 年冠状病毒病(COVID-19)是急性呼吸窘迫综合征(ARDS)的新病因。在多种病因的 ARDS 患者中,广泛使用无创通气(NIV)。实际上,由于 COVID-19 大流行导致 ARDS 病例增加,其在医院病房中的使用显着增加。但是,尚无证据支持 NIV 治疗 COVID-19 ARDS 的疗效。材料与方法:我们进行了一项观察性队列研究,纳入了在意大利罗马的一家三级 COVID 中心住院的成人 COVID-19 ARDS 患者。该研究分析了 28 天内从开始 NIV 起发生气管插管和/或死亡定义的 NIV 失败的发生率,其有效性以及相关的死亡相对风险。通过逻辑回归分析确定与结局相关的因素。结果:在研究期间,共有 942 名 COVID-19 患者被收入我院,其中 307 名(32.5%)在入院时患有 ARDS。在住院期间,有 224 名(23.8%)接受了 NIV 治疗。有 84 名(37.5%)患者发生了 NIV 失败。从开始 NIV 起 28 天,中度和重度 ARDS 的 NIV 失败的独立风险增加了五倍和二十倍(调整后的优势比,aOR=5.01,95%CI 2.08-12.09,19.95,95%CI 5.31-74.94)与轻度 ARDS 患者相比。共有 128 名患者(13.5%)被收入重症监护病房(ICU)。从 ICU 入院到 28 天,接受早期 NIV 治疗的气管插管 COVID-19 患者的死亡率降低了 40%(aOR 0.60,95%CI 0.25-1.46,p=0.010)与未进行 NIV 治疗的患者相比。结论:这些发现表明,NIV 失败与 COVID-19 ARDS 的严重程度类别独立相关。在轻度 ARDS(P/F>200mmHg)的 COVID-19 患者中开始 NIV 似乎增加了 NIV 的有效性,并降低了气管插管和/或死亡的风险。此外,早期 NIV(P/F>200mmHg)治疗似乎降低了从 ICU 入院到 28 天的 ICU 死亡率的风险。