Cammarota Gianmaria, Esposito Teresa, Azzolina Danila, Cosentini Roberto, Menzella Francesco, Aliberti Stefano, Coppadoro Andrea, Bellani Giacomo, Foti Giuseppe, Grasselli Giacomo, Cecconi Maurizio, Pesenti Antonio, Vitacca Michele, Lawton Tom, Ranieri V Marco, Di Domenico Sandro Luigi, Resta Onofrio, Gidaro Antonio, Potalivo Antonella, Nardi Giuseppe, Brusasco Claudia, Tesoro Simonetta, Navalesi Paolo, Vaschetto Rosanna, De Robertis Edoardo
Department of Medicine and Surgery, University of Perugia, Piazza Università 1, 06123, Perugia, Italy.
Department of Translational Medicine, University of Eastern Piedmont, Novara, Italy.
Crit Care. 2021 Jul 30;25(1):268. doi: 10.1186/s13054-021-03697-0.
Noninvasive respiratory support (NIRS) has been diffusely employed outside the intensive care unit (ICU) to face the high request of ventilatory support due to the massive influx of patients with acute respiratory failure (ARF) caused by coronavirus-19 disease (COVID-19). We sought to summarize the evidence on clinically relevant outcomes in COVID-19 patients supported by NIV outside the ICU.
We searched PUBMED®, EMBASE®, and the Cochrane Controlled Clinical trials register, along with medRxiv and bioRxiv repositories for pre-prints, for observational studies and randomized controlled trials, from inception to the end of February 2021. Two authors independently selected the investigations according to the following criteria: (1) observational study or randomized clinical trials enrolling ≥ 50 hospitalized patients undergoing NIRS outside the ICU, (2) laboratory-confirmed COVID-19, and (3) at least the intra-hospital mortality reported. Preferred Reporting Items for Systematic reviews and Meta-analysis guidelines were followed. Data extraction was independently performed by two authors to assess: investigation features, demographics and clinical characteristics, treatments employed, NIRS regulations, and clinical outcomes. Methodological index for nonrandomized studies tool was applied to determine the quality of the enrolled studies. The primary outcome was to assess the overall intra-hospital mortality of patients under NIRS outside the ICU. The secondary outcomes included the proportions intra-hospital mortalities of patients who underwent invasive mechanical ventilation following NIRS failure and of those with 'do-not-intubate' (DNI) orders.
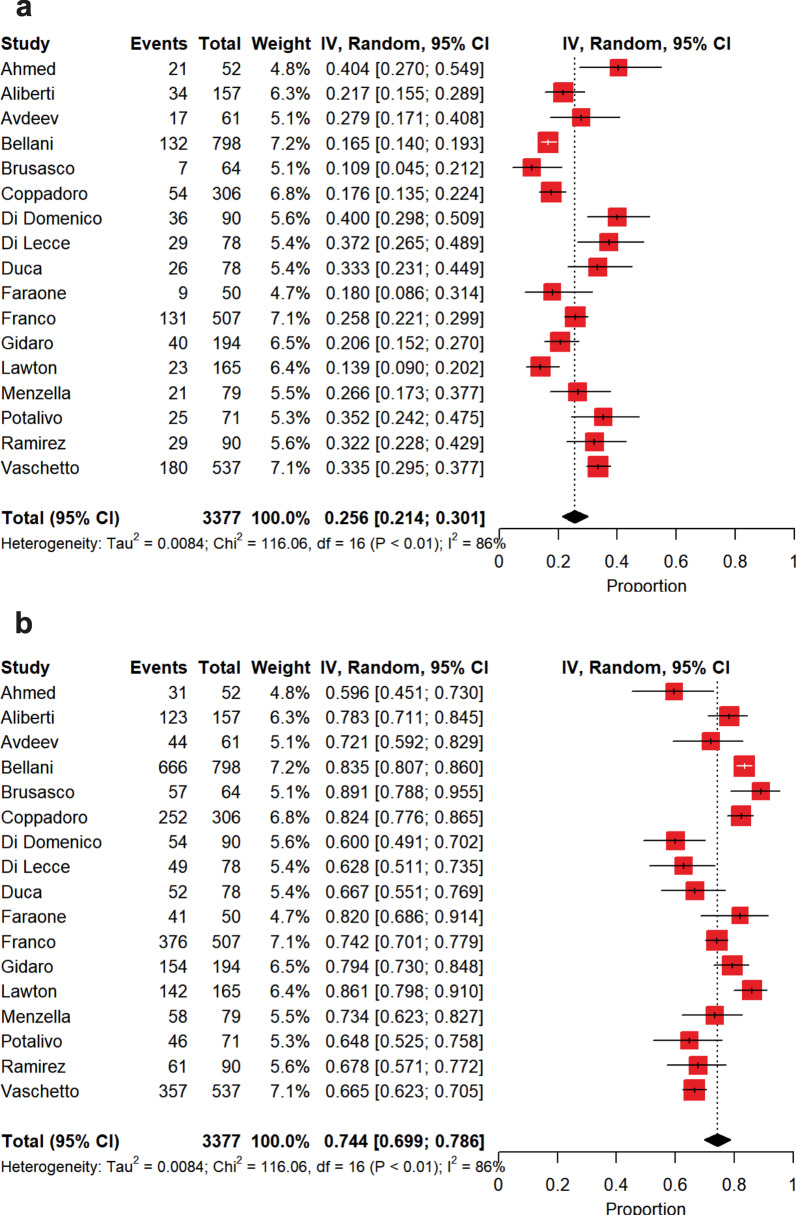
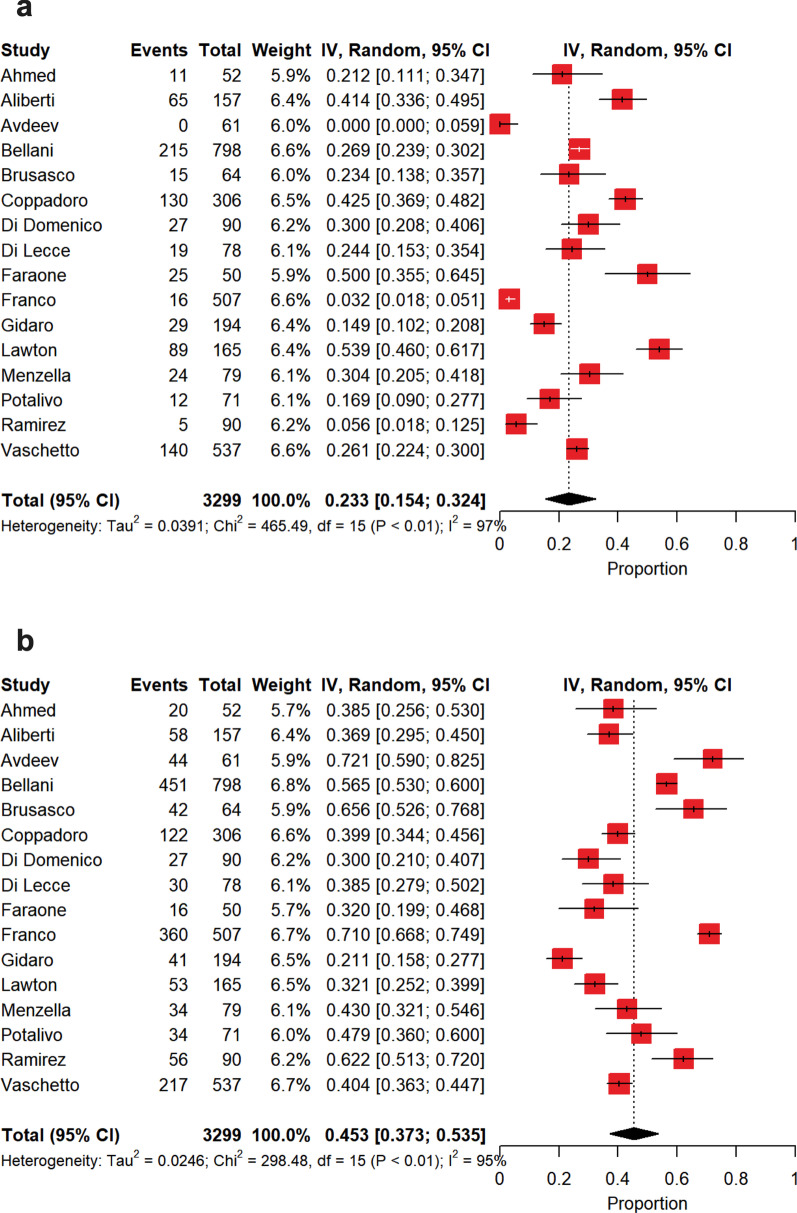
Seventeen investigations (14 peer-reviewed and 3 pre-prints) were included with a low risk of bias and a high heterogeneity, for a total of 3377 patients. The overall intra-hospital mortality of patients receiving NIRS outside the ICU was 36% [30-41%]. 26% [21-30%] of the patients failed NIRS and required intubation, with an intra-hospital mortality rising to 45% [36-54%]. 23% [15-32%] of the patients received DNI orders with an intra-hospital mortality of 72% [65-78%]. Oxygenation on admission was the main source of between-study heterogeneity.
During COVID-19 outbreak, delivering NIRS outside the ICU revealed as a feasible strategy to cope with the massive demand of ventilatory assistance.
PROSPERO, https://www.crd.york.ac.uk/prospero/ , CRD42020224788, December 11, 2020.
由于新型冠状病毒肺炎(COVID-19)导致急性呼吸衰竭(ARF)患者大量涌入,无创呼吸支持(NIRS)已在重症监护病房(ICU)外广泛应用,以应对通气支持的高需求。我们试图总结关于在ICU外接受无创通气(NIV)支持的COVID-19患者临床相关结局的证据。
我们检索了PUBMED®、EMBASE®和Cochrane对照临床试验注册库,以及medRxiv和bioRxiv预印本库,以查找从创刊到2021年2月底的观察性研究和随机对照试验。两位作者根据以下标准独立选择研究:(1)观察性研究或随机临床试验,纳入≥50例在ICU外接受NIRS的住院患者;(2)实验室确诊的COVID-19;(3)至少报告了院内死亡率。遵循系统评价和Meta分析的首选报告项目指南。由两位作者独立进行数据提取,以评估:研究特征、人口统计学和临床特征、采用的治疗方法、NIRS参数以及临床结局。应用非随机研究方法学指数工具来确定纳入研究的质量。主要结局是评估ICU外接受NIRS患者的总体院内死亡率。次要结局包括NIRS失败后接受有创机械通气患者的院内死亡率以及有“不插管”(DNI)医嘱患者的院内死亡率。
共纳入17项研究(14项同行评审研究和3篇预印本),偏倚风险低但异质性高,共3377例患者。在ICU外接受NIRS患者的总体院内死亡率为36%[30 - 41%]。26%[21 - 30%]的患者NIRS失败需要插管,院内死亡率升至45%[36 - 54%]。23%[15 - 32%]的患者接受了DNI医嘱,院内死亡率为72%[65 - 78%]。入院时的氧合情况是研究间异质性的主要来源。
在COVID-19疫情期间,在ICU外提供NIRS是应对通气支持巨大需求的一种可行策略。
PROSPERO,https://www.crd.york.ac.uk/prospero/ ,CRD42020224788,2020年12月11日。