Steinkirchner Anna B, Zimmermann Martina E, Donhauser Ferdinand J, Dietl Alexander, Brandl Caroline, Koller Michael, Loss Julika, Heid Iris M, Stark Klaus J
Department of Genetic Epidemiology, University of Regensburg, Regensburg, Germany.
Department of Internal Medicine II, University Hospital Regensburg, Regensburg, Germany.
J Epidemiol Community Health. 2022 Aug 26;76(11):931-8. doi: 10.1136/jech-2022-219096.
To estimate prevalence and incidence of diseases through self-reports in observational studies, it is important to understand the accuracy of participant reports. We aimed to quantify the agreement of self-reported and general practitioner-reported diseases in an old-aged population and to identify socio-demographic determinants of agreement.
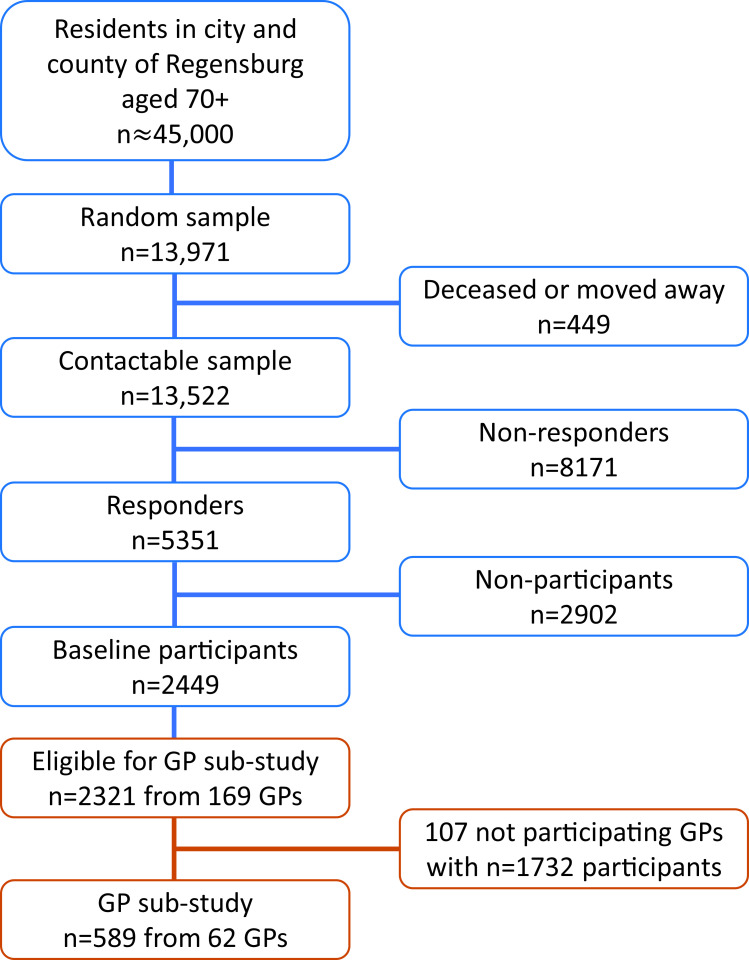
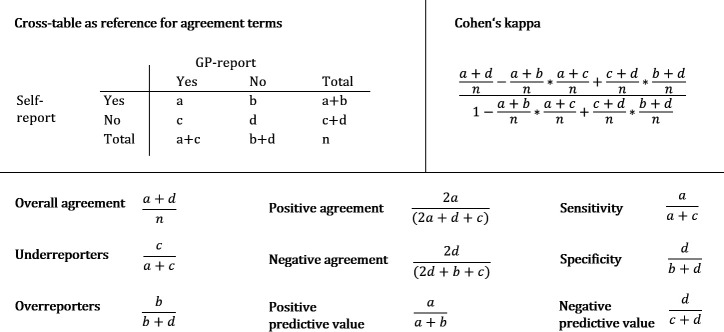
This analysis was conducted as part of the AugUR study (n=2449), a prospective population-based cohort study in individuals aged 70-95 years, including 2321 participants with consent to contact physicians. Self-reported chronic diseases of participants were compared with medical data provided by their respective general practitioners (n=589, response rate=25.4%). We derived overall agreement, over-reporting/under-reporting, and Cohen's kappa and used logistic regression to evaluate the dependency of agreement on participants' sociodemographic characteristics.
Among the 589 participants (53.1% women), 96.9% reported at least one of the evaluated chronic diseases. Overall agreement was >80% for hypertension, diabetes, myocardial infarction, stroke, cancer, asthma, bronchitis/chronic obstructive pulmonary disease and rheumatoid arthritis, but lower for heart failure, kidney disease and arthrosis. Cohen's kappa was highest for diabetes and cancer and lowest for heart failure, musculoskeletal, kidney and lung diseases. Sex was the primary determinant of agreement on stroke, kidney disease, cancer and rheumatoid arthritis. Agreement for myocardial infarction and stroke was most compromised by older age and for cancer by lower educational level.
Self-reports may be an effective tool to assess diabetes and cancer in observational studies in the old and very old aged. In contrast, self-reports on heart failure, musculoskeletal, kidney or lung diseases may be substantially imprecise.
在观察性研究中,通过自我报告来估计疾病的患病率和发病率时,了解参与者报告的准确性很重要。我们旨在量化老年人群中自我报告疾病与全科医生报告疾病之间的一致性,并确定一致性的社会人口学决定因素。
本分析是AugUR研究(n = 2449)的一部分,这是一项基于人群的前瞻性队列研究,研究对象为70 - 95岁的个体,其中2321名参与者同意联系医生。将参与者自我报告的慢性病与各自全科医生提供的医疗数据进行比较(n = 589,回复率 = 25.4%)。我们得出总体一致性、过度报告/漏报情况以及科恩kappa系数,并使用逻辑回归来评估一致性对参与者社会人口学特征的依赖性。
在589名参与者(53.1%为女性)中,96.9%报告了至少一种评估的慢性病。高血压、糖尿病、心肌梗死、中风、癌症、哮喘、支气管炎/慢性阻塞性肺疾病和类风湿关节炎的总体一致性>80%,但心力衰竭、肾病和关节病的一致性较低。糖尿病和癌症的科恩kappa系数最高,心力衰竭、肌肉骨骼疾病、肾病和肺病的最低。性别是中风、肾病、癌症和类风湿关节炎一致性的主要决定因素。年龄较大对心肌梗死和中风的一致性影响最大,教育水平较低对癌症的一致性影响最大。
在针对老年人和高龄老人的观察性研究中,自我报告可能是评估糖尿病和癌症的有效工具。相比之下,关于心力衰竭、肌肉骨骼疾病、肾病或肺病的自我报告可能存在较大不准确性。