Center for Health Equity, Northern Arizona University, Flagstaff, Arizona; Department of Epidemiology, University of North Carolina, Chapel Hill, North Carolina, United States of America.
Department of Epidemiology, University of North Carolina, Chapel Hill, North Carolina, United States of America.
J Card Fail. 2017 Nov;23(11):802-808. doi: 10.1016/j.cardfail.2017.09.002. Epub 2017 Sep 8.
The aim of this work was to estimate agreement of self-reported heart failure (HF) with physician-diagnosed HF and compare the prevalence of HF according to method of ascertainment.
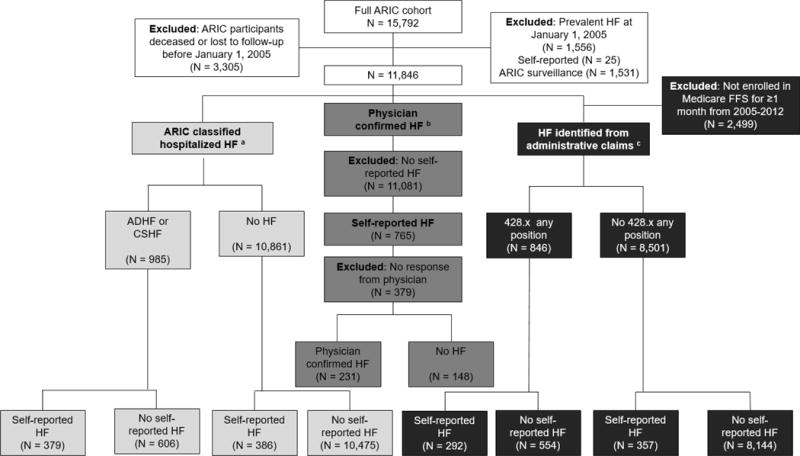
ARIC cohort members (60-83 years of age) were asked annually whether a physician indicated that they have HF. For those self-reporting HF, physicians were asked to confirm their patients' HF status. Physician-diagnosed HF included surveillance of hospitalized HF and hospitalized and outpatient HF identified in administrative claims databases. We estimated sensitivity, specificity, positive predicted value, kappa, prevalence and bias-adjusted kappa (PABAK), and prevalence. Compared with physician-diagnosed HF, sensitivity of self-report was low (28%-38%) and specificity was high (96%-97%). Agreement was poor (kappa 0.32-0.39) and increased when adjusted for prevalence and bias (PABAK 0.73-0.83). Prevalence of HF measured by self-report (9.0%), ARIC-classified hospitalizations (11.2%), and administrative hospitalization claims (12.7%) were similar. When outpatient HF claims were included, prevalence of HF increased to 18.6%.
For accurate estimates HF burden, self-reports of HF are best confirmed by means of appropriate diagnostic tests or medical records. Our results highlight the need for improved awareness and understanding of HF by patients, because accurate patient awareness of the diagnosis may enhance management of this common condition.
本研究旨在评估自我报告的心衰(HF)与医生诊断的心衰的一致性,并比较两种方法确定心衰的患病率。
ARIC 队列成员(60-83 岁)每年被问及是否有医生表示他们有心衰。对于自我报告 HF 的患者,医生被要求确认其患者的心衰状况。医生诊断的心衰包括住院心衰监测以及在行政索赔数据库中识别的住院和门诊心衰。我们估计了敏感性、特异性、阳性预测值、kappa、患病率和偏倚调整 kappa(PABAK)以及患病率。与医生诊断的心衰相比,自我报告的敏感性较低(28%-38%),特异性较高(96%-97%)。一致性较差(kappa 值为 0.32-0.39),当调整患病率和偏倚时,一致性增加(PABAK 值为 0.73-0.83)。通过自我报告(9.0%)、ARIC 分类住院(11.2%)和行政住院索赔(12.7%)测量的 HF 患病率相似。当包括门诊 HF 索赔时,HF 的患病率增加到 18.6%。
为了准确估计 HF 负担,HF 的自我报告最好通过适当的诊断测试或医疗记录进行确认。我们的研究结果强调了患者对 HF 的认识和理解需要提高,因为患者对诊断的准确认识可能会增强对这种常见疾病的管理。