Zhang Ting, Mei Qimin, Dai Shabai, Liu Yecheng, Zhu Huadong
Emergency Department, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Science and Peking Union Medical College, Beijing, China.
Department of Family Medicine & Division of General Internal Medicine, Department of Medicine, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, China.
Ann Intensive Care. 2022 Aug 27;12(1):81. doi: 10.1186/s13613-022-01052-2.
Dexmedetomidine is widely used in patients with sepsis. However, its effect on septic patients remains controversial. The objective of this study was to summarize all randomized controlled trials (RCTs) examining dexmedetomidine use in sepsis patients.
This systematic review and meta-analysis included RCTs comparing dexmedetomidine with other sedatives in adult sepsis patients. We generated pooled relative risks (RRs) and standardized mean differences and performed trial sequential analysis and a cumulative meta-analysis. The primary outcome was mortality, and the secondary outcomes were the length of the intensive care unit stay, duration of mechanical ventilation, number of ventilation-free days, incidence of total adverse event, incidence of delirium, and levels of interleukin 6, tumor necrosis factor alpha, and alanine aminotransferase.
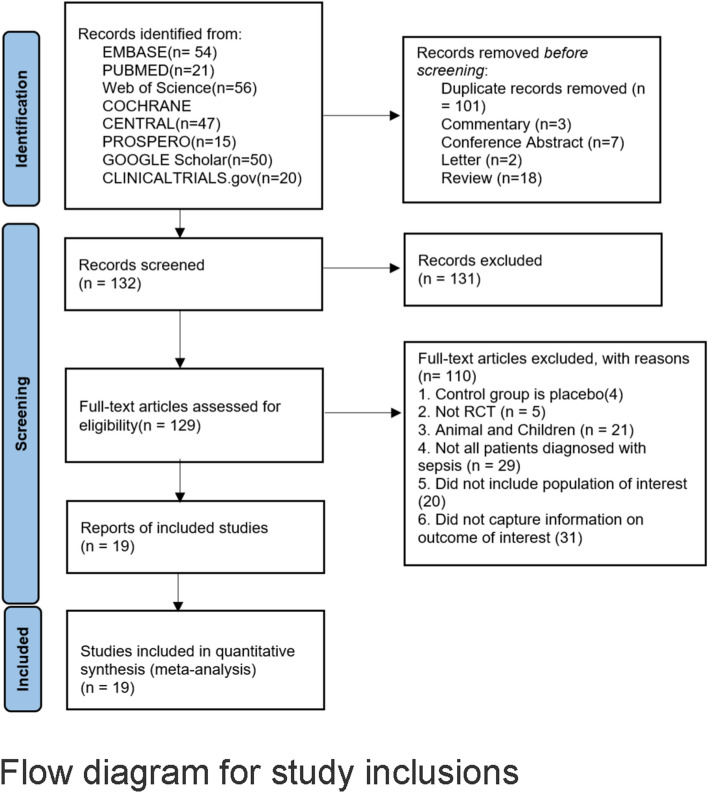
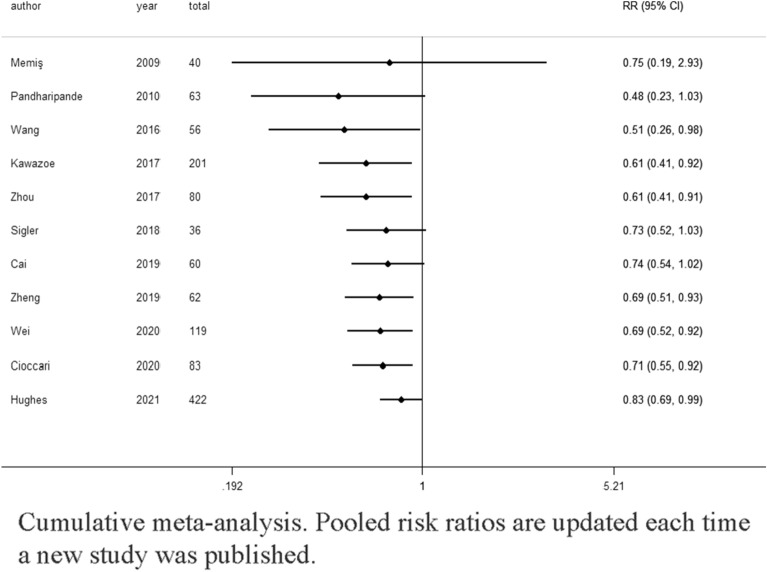
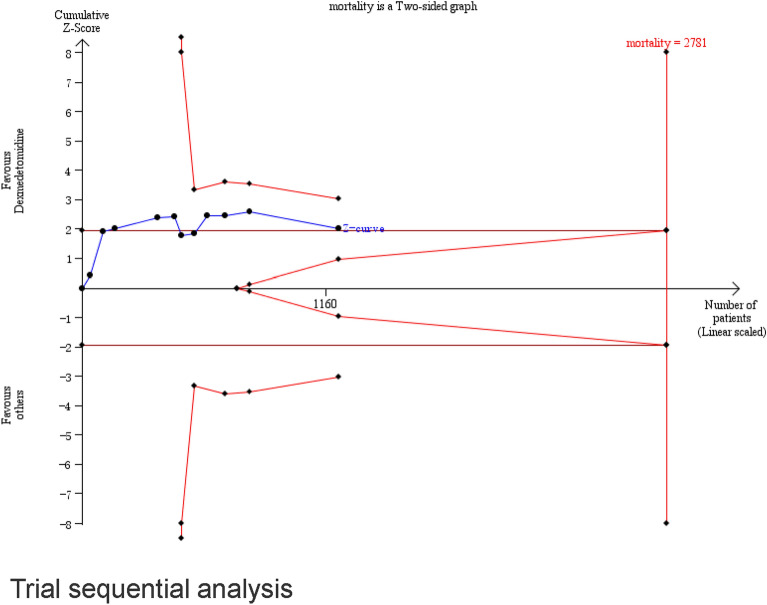
We included 19 RCTs that enrolled 1929 patients. Compared with other sedatives, dexmedetomidine decreased the all-cause mortality (RR 0.83; 95% confidence interval [CI] [0.69, 0.99]) and inflammatory response (interleukin 6 and tumor necrosis factor alpha levels at 24 h: standardized mean difference (SMD) - 2.15; 95% CI [- 3.25, - 1.05] and SMD - 1.07, 95% CI [- 1.92, - 0.22], respectively). Trial sequential analysis showed that it is not up to required information size. The overall risk adverse events was similar between dexmedetomidine and the other sedatives (RR 1.27, 95% CI [0.69, 2.36]), but dexmedetomidine increased the risk of arrhythmias (RR 1.43, 95% CI [0.59, 3.51]). Length of intensive care unit stay (SMD - 0.22; 95% CI [- 0.85, - 0.41]), duration of mechanical ventilation (SMD 0.12; 95% CI [- 1.10, 1.35]), incidence of delirium (RR 0.98; 95% CI [0.72, 1.33]), and levels of alanine aminotransferase and creatinine at 24 h were not significantly reduced.
Dexmedetomidine in sepsis patients could significantly reduce mortality compared with benzodiazepines but not with propofol. In addition, dexmedetomidine can significantly decrease inflammatory response in patients with sepsis compared with other sedatives. Dexmedetomidine might lead to an increased incidence of arrhythmias, but its safety profile did not show significant differences in the incidence of total adverse events. Future RCTs are needed to determine the sepsis patient population that would benefit most from dexmedetomidine and its optimal dosing regimen.
右美托咪定广泛应用于脓毒症患者。然而,其对脓毒症患者的疗效仍存在争议。本研究的目的是总结所有考察右美托咪定在脓毒症患者中应用的随机对照试验(RCT)。
本系统评价和荟萃分析纳入了在成年脓毒症患者中比较右美托咪定与其他镇静剂的RCT。我们生成了合并相对危险度(RR)和标准化均数差,并进行了试验序贯分析和累积荟萃分析。主要结局为死亡率,次要结局为重症监护病房住院时间、机械通气时间、无通气天数、总不良事件发生率、谵妄发生率以及白细胞介素6、肿瘤坏死因子α和丙氨酸转氨酶水平。
我们纳入了19项RCT,共1929例患者。与其他镇静剂相比,右美托咪定降低了全因死亡率(RR 0.83;95%置信区间[CI][0.69,0.99])和炎症反应(24小时时白细胞介素6和肿瘤坏死因子α水平:标准化均数差(SMD)-2.15;95%CI[-3.25,-1.05]和SMD -1.07,95%CI[-1.92,-0.22])。试验序贯分析表明,未达到所需信息量。右美托咪定与其他镇静剂的总体不良事件风险相似(RR 1.27,95%CI[0.69,2.36]),但右美托咪定增加了心律失常风险(RR 1.43,95%CI[0.59,3.51])。重症监护病房住院时间(SMD -0.22;9-five%CI[-0.85,-0.41])、机械通气时间(SMD 0.12;95%CI[-1.10,1.35])、谵妄发生率(RR 0.98;95%CI[0.72,1.33])以及24小时时丙氨酸转氨酶和肌酐水平未显著降低。
与苯二氮䓬类药物相比,脓毒症患者使用右美托咪定可显著降低死亡率,但与丙泊酚相比则不然。此外,与其他镇静剂相比,右美托咪定可显著降低脓毒症患者的炎症反应。右美托咪定可能导致心律失常发生率增加,但其安全性在总不良事件发生率方面未显示出显著差异。未来需要进行RCT以确定最能从右美托咪定及其最佳给药方案中获益的脓毒症患者群体。