BHF Glasgow Cardiovascular Research Centre, School of Cardiovascular and Metabolic Health, University of Glasgow, Glasgow, UK.
Cardiovascular Division, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
Nat Med. 2022 Sep;28(9):1956-1964. doi: 10.1038/s41591-022-01971-4. Epub 2022 Aug 27.
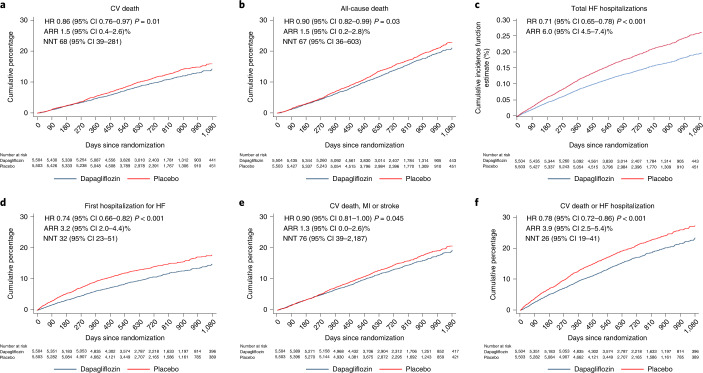
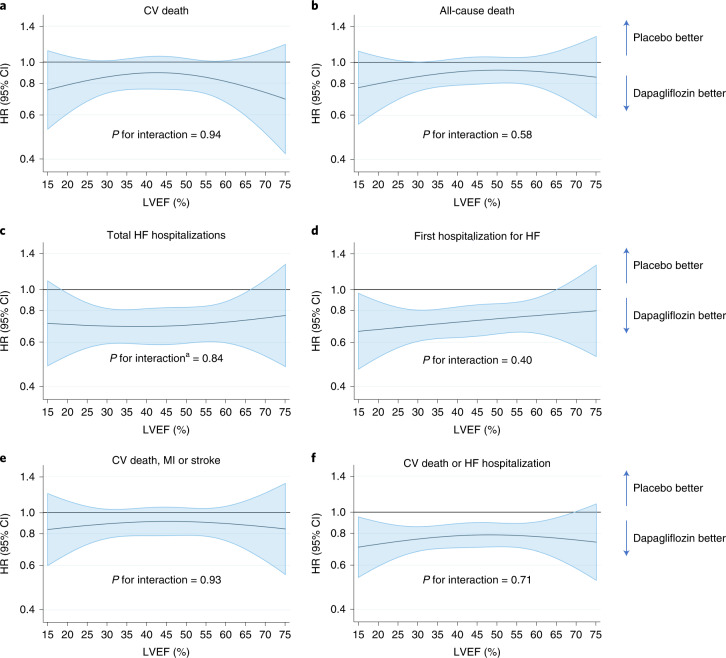
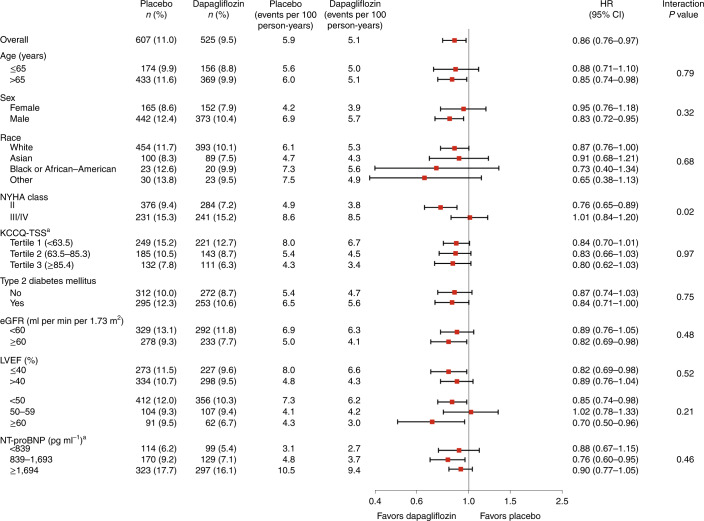
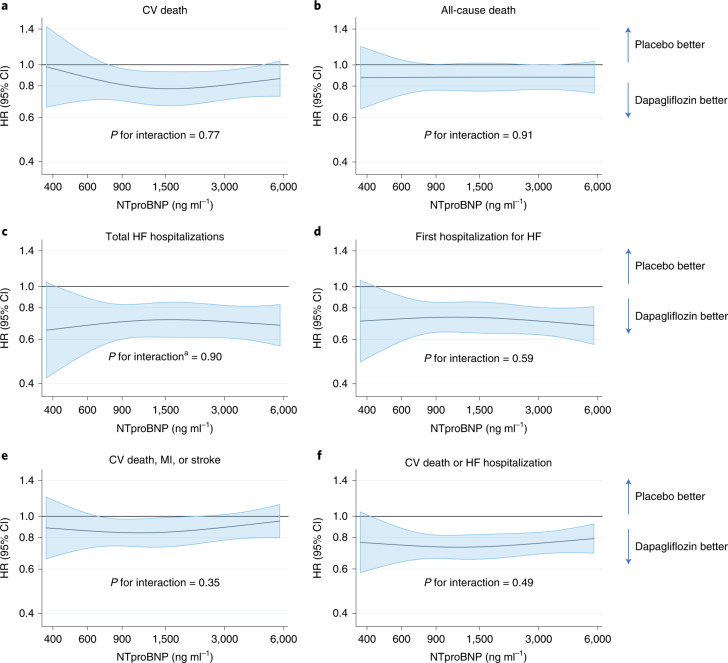
Whether the sodium-glucose cotransporter 2 inhibitor dapagliflozin reduces the risk of a range of morbidity and mortality outcomes in patients with heart failure regardless of ejection fraction is unknown. A patient-level pooled meta-analysis of two trials testing dapagliflozin in participants with heart failure and different ranges of left ventricular ejection fraction (≤40% and >40%) was pre-specified to examine the effect of treatment on endpoints that neither trial, individually, was powered for and to test the consistency of the effect of dapagliflozin across the range of ejection fractions. The pre-specified endpoints were: death from cardiovascular causes; death from any cause; total hospital admissions for heart failure; and the composite of death from cardiovascular causes, myocardial infarction or stroke (major adverse cardiovascular events (MACEs)). A total of 11,007 participants with a mean ejection fraction of 44% (s.d. 14%) were included. Dapagliflozin reduced the risk of death from cardiovascular causes (hazard ratio (HR) 0.86, 95% confidence interval (CI) 0.76-0.97; P = 0.01), death from any cause (HR 0.90, 95% CI 0.82-0.99; P = 0.03), total hospital admissions for heart failure (rate ratio 0.71, 95% CI 0.65-0.78; P < 0.001) and MACEs (HR 0.90, 95% CI 0.81-1.00; P = 0.045). There was no evidence that the effect of dapagliflozin differed by ejection fraction. In a patient-level pooled meta-analysis covering the full range of ejection fractions in patients with heart failure, dapagliflozin reduced the risk of death from cardiovascular causes and hospital admissions for heart failure (PROSPERO: CRD42022346524).
无论钠-葡萄糖共转运蛋白 2 抑制剂达格列净是否降低射血分数不同的心力衰竭患者的一系列发病率和死亡率结局的风险尚不清楚。对两项测试达格列净在射血分数不同(≤40%和>40%)的心力衰竭患者中疗效的试验进行了患者水平的合并荟萃分析,预先设定了检查该治疗对每个试验均无足够效能评估的终点的效果,并检验了达格列净在整个射血分数范围内的效果一致性。预先设定的终点是:心血管原因导致的死亡;任何原因导致的死亡;心力衰竭的总住院次数;以及心血管原因导致的死亡、心肌梗死或中风的综合指标(主要不良心血管事件(MACE))。共有 11007 名平均射血分数为 44%(标准差 14%)的患者入组。达格列净降低了心血管原因导致的死亡风险(风险比(HR)0.86,95%置信区间(CI)0.76-0.97;P=0.01)、任何原因导致的死亡风险(HR 0.90,95% CI 0.82-0.99;P=0.03)、心力衰竭的总住院次数(率比 0.71,95% CI 0.65-0.78;P<0.001)和 MACEs(HR 0.90,95% CI 0.81-1.00;P=0.045)。没有证据表明达格列净的效果与射血分数不同。在涵盖心力衰竭患者整个射血分数范围的患者水平合并荟萃分析中,达格列净降低了心血管原因导致的死亡和心力衰竭的住院风险(PROSPERO:CRD42022346524)。