Department of Internal Medicine, Division of Endocrinology, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Division of Endocrinology, NYU Langone Medical Center/ Bellevue Hospital Center, New York, NY.
J Clin Endocrinol Metab. 2022 Nov 23;107(11):3162-3174. doi: 10.1210/clinem/dgac492.
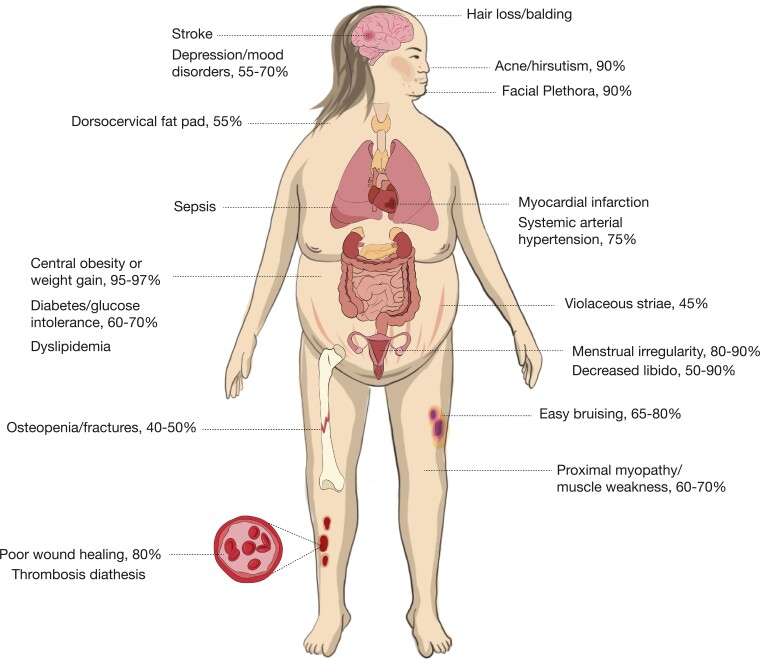
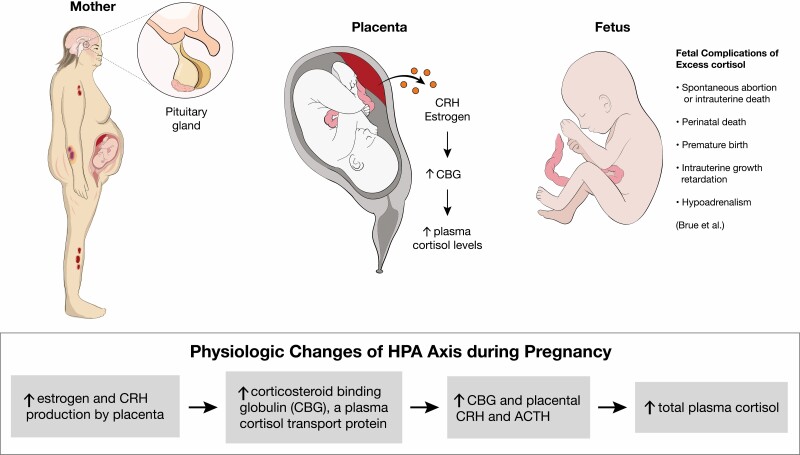
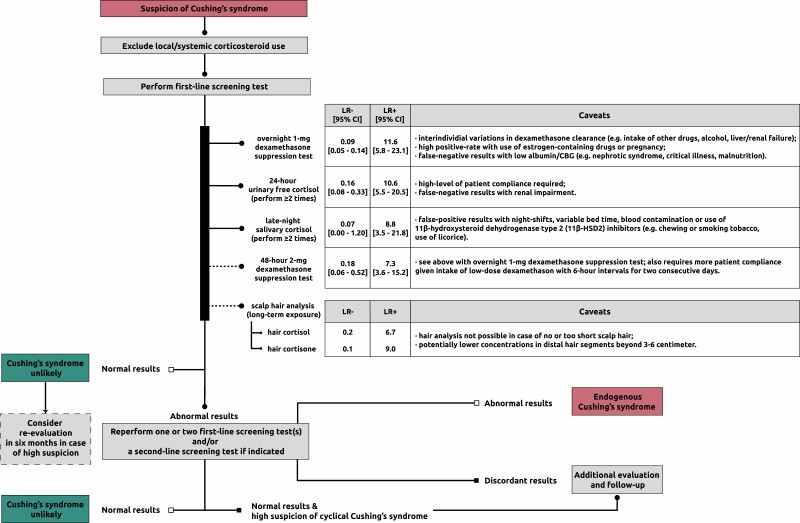
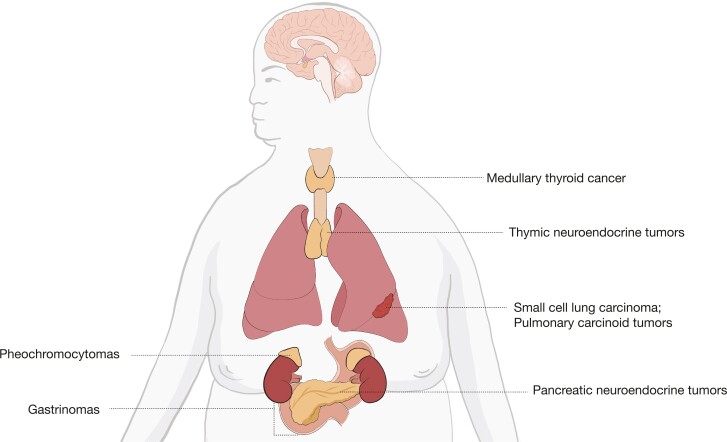
Cushing syndrome results from supraphysiological exposure to glucocorticoids and is associated with significant morbidity and mortality. The pathogenesis includes administration of corticosteroids (exogenous Cushing syndrome) or autonomous cortisol overproduction, whether or not ACTH-dependent (endogenous Cushing syndrome). An early diagnosis of Cushing syndrome is warranted; however, in clinical practice, it is very challenging partly because of resemblance with other common conditions (ie, pseudo-Cushing syndrome). Initial workup should start with excluding local and systemic corticosteroid use. First-line screening tests including the 1-mg dexamethasone suppression test, 24-hour urinary free cortisol excretion, and late-night salivary cortisol measurement should be performed to screen for endogenous Cushing syndrome. Scalp-hair cortisol/cortisone analysis helps in the assessment of long-term glucocorticoid exposure as well as in detection of transient periods of hypercortisolism as observed in cyclical Cushing syndrome. Interpretation of results can be difficult because of individual patient characteristics and hence requires awareness of test limitations. Once endogenous Cushing syndrome is established, measurement of plasma ACTH concentrations differentiates between ACTH-dependent (80%-85%) or ACTH-independent (15%-20%) causes. Further assessment with different imaging modalities and dynamic biochemical testing including bilateral inferior petrosal sinus sampling helps further pinpoint the cause of Cushing's syndrome. In this issue of "Approach to the patient," the diagnostic workup of Cushing syndrome is discussed with answering the questions when to screen, how to screen, and how to differentiate the different causes. In this respect, the latest developments in biochemical and imaging techniques are discussed as well.
库欣综合征是由于糖皮质激素的生理水平以上暴露引起的,与显著的发病率和死亡率有关。其发病机制包括皮质类固醇(外源性库欣综合征)或自主皮质醇过度产生,无论是否依赖 ACTH(内源性库欣综合征)。库欣综合征的早期诊断是必要的;然而,在临床实践中,这是非常具有挑战性的,部分原因是它与其他常见疾病(即假性库欣综合征)相似。初步检查应从排除局部和全身皮质类固醇的使用开始。应进行一线筛查试验,包括 1 毫克地塞米松抑制试验、24 小时尿游离皮质醇排泄和夜间唾液皮质醇测量,以筛查内源性库欣综合征。头皮毛发皮质醇/皮质酮分析有助于评估长期糖皮质激素暴露,以及检测到在周期性库欣综合征中观察到的短暂高皮质醇血症。由于个体患者的特征,结果的解释可能很困难,因此需要了解测试的局限性。一旦确定了内源性库欣综合征,测量血浆 ACTH 浓度可区分 ACTH 依赖性(80%-85%)或 ACTH 独立性(15%-20%)的原因。通过不同的成像方式和动态生化测试(包括双侧岩下窦取样)进一步评估有助于进一步确定库欣综合征的原因。在本期“患者处理方法”中,讨论了库欣综合征的诊断检查,回答了何时进行筛查、如何进行筛查以及如何区分不同原因的问题。在这方面,还讨论了生化和成像技术的最新进展。