Department of Cardiac Surgery, Harefield Hospital, Royal Brompton and Harefield Hospitals, Part of Guy's and St. Thomas' NHS Foundation Trust, London, UK.
Department of Pharmacology, Zagreb University School of Medicine, Zagreb, Croatia.
J Card Surg. 2022 Nov;37(11):3801-3810. doi: 10.1111/jocs.16888. Epub 2022 Aug 30.
Although concomitant pulmonary vein isolation (PVI) is used more frequently than the Cox-Maze procedure, which is currently the gold standard treatment for atrial fibrillation (AF), data on the comparative effectiveness of the two procedures after concomitant mitral valve (MV) surgery are still limited.
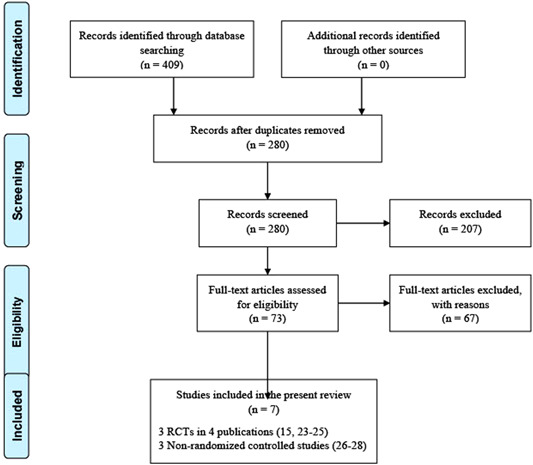
We conducted a systematic review to identify randomized controlled trials (RCTs) and observational studies comparing the mid-term mortality and recurrence of AF after concomitant Cox-Maze and PVI in patients with AF undergoing MV surgery based on 12-month follow-up.
Medline, EMBASE databases, and the Cochrane Library were searched from 1987 up to March 2022 for studies comparing concomitant Cox-Maze and PVI. Additionally, a meta-analysis of RCTs was performed to compare the mid-term clinical outcomes between these two surgical ablation techniques.
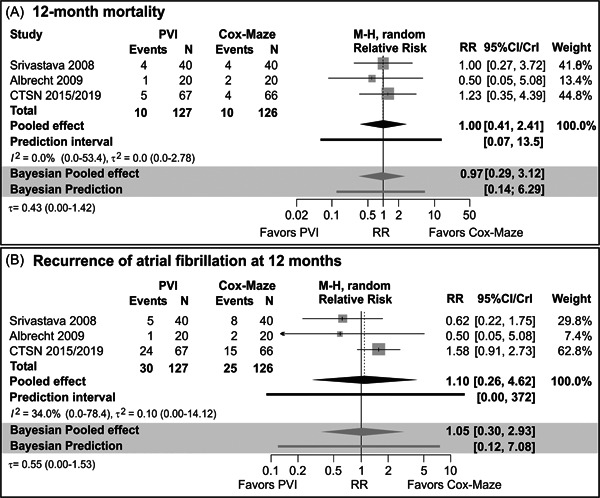
Three RCTs and three observational studies meeting the inclusion criteria were included in this systematic review with 790 patients in total (532 concomitant Cox-Maze and 258 PVI during MV surgery). Most studies reported that the concomitant Cox-Maze procedure was associated with higher freedom from AF at 12-month follow-up than PVI. Regarding AF recurrence, estimates pooled across the three RCTs indicated large heterogeneity and high uncertainty. In the largest and highest quality RCT, 12-month AF recurrence was higher in the PVI arm (risk ratio = 1.58, 95% CI: 0.91-2.73). In two out of three higher-quality observational studies, 12-month AF recurrence was higher in PVI than in the Cox-Maze arm (estimated adjusted probabilities 11% vs. 8% and 35% vs. 17%, respectively). RCTs demonstrated comparable 12-month mortality between concomitant Cox-Maze and PVI, while observational studies demonstrated the survival benefit of Cox-Maze.
Concomitant Cox-Maze in AF patients undergoing MV surgery is associated with better mid-term freedom from AF when compared to PVI with comparable mid-term survival. Large observational studies suggest that there might be a mid-term survival benefit among patients after concomitant Cox-Maze. Further large RCTs with longer standardized follow-up are required to clarify the benefits of concomitant Cox-Maze in AF patients during MV surgery.
尽管同期肺静脉隔离(PVI)比目前房颤(AF)的金标准治疗——迷宫手术更为常用,但同期行二尖瓣(MV)手术时两种术式的中期死亡率和 AF 复发的数据仍有限。
我们进行了一项系统评价,以确定基于 12 个月随访的比较同期行迷宫手术和 PVI 治疗 MV 术后 AF 患者的中期死亡率和 AF 复发的随机对照试验(RCT)和观察性研究。
从 1987 年至 2022 年 3 月,我们检索了 Medline、EMBASE 数据库和 Cochrane 图书馆,以确定比较同期行迷宫手术和 PVI 的研究。此外,我们还对 RCT 进行了荟萃分析,以比较这两种手术消融技术的中期临床结局。
这项系统评价共纳入了 3 项 RCT 和 3 项符合纳入标准的观察性研究,共计 790 例患者(同期行 MV 手术的 532 例行迷宫手术,258 例行 PVI)。大多数研究报告称,同期行迷宫手术的患者在 12 个月随访时无 AF 的比例更高。关于 AF 复发,跨 3 项 RCT 的汇总估计存在较大异质性和高度不确定性。在最大和质量最高的 RCT 中,PVI 组的 12 个月 AF 复发率更高(风险比=1.58,95%CI:0.91-2.73)。在 3 项高质量观察性研究中的 2 项中,PVI 组的 12 个月 AF 复发率高于迷宫手术组(估计调整概率分别为 11% vs. 8%和 35% vs. 17%)。RCT 表明同期行迷宫手术和 PVI 的患者 12 个月死亡率相当,而观察性研究表明迷宫手术有生存获益。
同期行 MV 手术的 AF 患者中,与同期行 PVI 相比,迷宫手术与中期生存率相当,但 AF 无复发的中期获益更好。大型观察性研究表明,同期行迷宫手术的患者可能有中期生存获益。需要进一步开展大型 RCT,进行更标准化的随访,以明确同期行迷宫手术对 MV 术后 AF 患者的获益。