Division of Medicine, Chumphonkatudomsak Hospital, Chumporn, Thailand.
Department of Research and Development, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
BMC Infect Dis. 2022 Aug 30;22(1):717. doi: 10.1186/s12879-022-07700-z.
Neurosyphilis (NS) can lead to acute ischemic stroke (AIS) or transient ischemic attack (TIA). We compared the clinical characteristics and laboratory features among AIS and TIA patients who were syphilis-seronegative (control group) or had latent syphilis (LS) or NS to evaluate their stroke outcome.
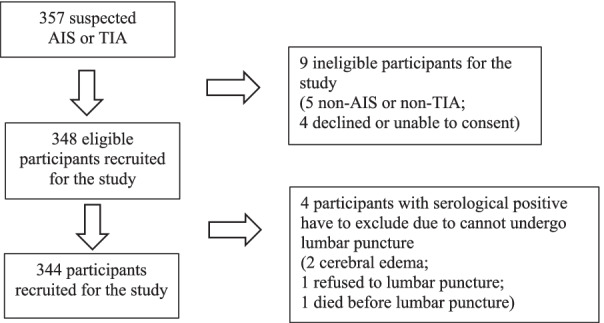
This prospective cohort study was conducted on patients who had recently suffered AIS or TIA. After serological syphilis screening, clinical and laboratory data were collected, and brain imaging and spinal tap (serologically syphilis-positive patients only) were performed. Stroke outcome was re-evaluated approximately three months later.
The 344 enrolled patients were divided into three groups: control group (83.7%), LS (13.1%), and NS (3.2%). A multivariate analysis revealed: 1) age of ≥ 70 years, generalized brain atrophy via imaging, and alopecia (adjusted odds ratio [AOR] = 2.635, 2.415, and 13.264, respectively) were significantly associated with LS vs controls; 2) age of ≥ 70 years (AOR = 14.633) was significantly associated with NS vs controls; and 3) the proportion of patients with dysarthria was significantly lower (AOR = 0.154) in the NS group than in the LS group. Regarding the NS patient cerebrospinal fluid (CSF) profile, only 2/11 cases had positive CSF-Venereal Disease Research Laboratory (VDRL) test results; the other nine cases were diagnosed from elevated white blood cell counts or protein levels combined with positive CSF fluorescent treponemal antibody absorption (FTA-ABS) test results. Regarding disability, the initial modified Rankin scale (mRS) score was lower in the control group than in the NS group (p = 0.022). At 3 months post-stroke, the mRS score had significantly decreased in the control (p < 0.001) and LS (p = 0.001) groups. Regarding activities of daily living, the 3-month Barthel Index (BI) score was significantly higher in control patients than in LS (p = 0.030) or NS (p = 0.002) patients. Additionally, the 3-month BI score was significantly increased in the control (p < 0.001) and LS (p = 0.001) groups.
Because syphilis was detected in many AIS and TIA patients, especially those aged ≥ 70 years, routine serological syphilis screening may be warranted in this population. Patients with syphilitic infection had worse stroke outcomes compared with NS patients.
神经梅毒(NS)可导致急性缺血性中风(AIS)或短暂性脑缺血发作(TIA)。我们比较了梅毒血清学阴性(对照组)或潜伏梅毒(LS)或 NS 的 AIS 和 TIA 患者的临床特征和实验室特征,以评估他们的中风结局。
这是一项前瞻性队列研究,纳入了近期发生 AIS 或 TIA 的患者。在进行血清梅毒筛查后,收集临床和实验室数据,并进行脑部成像和腰椎穿刺(仅用于血清学梅毒阳性患者)。大约三个月后再次评估中风结局。
纳入的 344 名患者分为三组:对照组(83.7%)、LS(13.1%)和 NS(3.2%)。多变量分析显示:1)年龄≥70 岁、影像学上存在广泛性脑萎缩和脱发(调整后的优势比[OR]分别为 2.635、2.415 和 13.264)与 LS 相比,与对照组显著相关;2)年龄≥70 岁(OR=14.633)与 NS 相比,与对照组显著相关;3)与 LS 组相比,NS 组构音障碍患者的比例明显更低(OR=0.154)。对于 NS 患者的脑脊液(CSF)特征,仅 2/11 例 CSF-性病研究实验室(VDRL)检测结果阳性;其他 9 例是根据白细胞计数升高或蛋白水平升高结合阳性 CSF 荧光密螺旋体抗体吸收(FTA-ABS)检测结果诊断的。关于残疾,对照组的初始改良 Rankin 量表(mRS)评分低于 NS 组(p=0.022)。中风后 3 个月,对照组(p<0.001)和 LS 组(p=0.001)的 mRS 评分均显著降低。关于日常生活活动,对照组患者的 3 个月巴氏指数(BI)评分明显高于 LS(p=0.030)或 NS(p=0.002)组。此外,对照组(p<0.001)和 LS 组(p=0.001)的 3 个月 BI 评分均显著升高。
由于在许多 AIS 和 TIA 患者中检测到梅毒,特别是年龄≥70 岁的患者,该人群可能需要常规进行血清学梅毒筛查。患有梅毒感染的患者与 NS 患者相比,中风结局更差。