Department of International Health, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland.
Marshfield Clinic Research Institute, Marshfield, Wisconsin.
JAMA Netw Open. 2022 Aug 1;5(8):e2227348. doi: 10.1001/jamanetworkopen.2022.27348.
Few studies have prospectively assessed SARS-CoV-2 community infection in children aged 0 to 4 years. Information about SARS-CoV-2 incidence and clinical and virological features in young children could help guide prevention and mitigation strategies.
To assess SARS-CoV-2 incidence, clinical and virological features, and symptoms in a prospective household cohort and to compare viral load by age group, symptoms, and SARS-CoV-2 lineage in young children, older children, and adults.
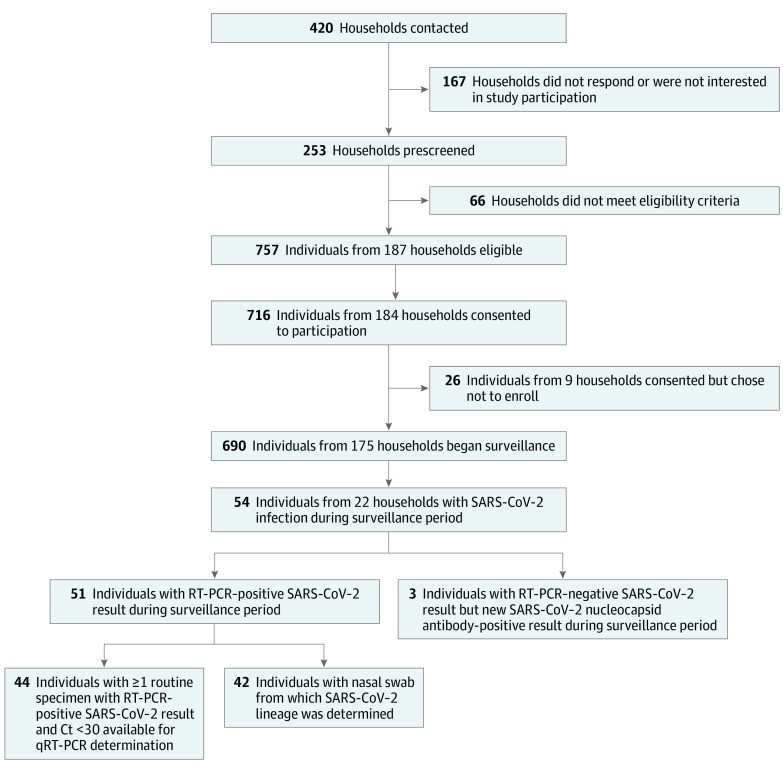
DESIGN, SETTING, AND PARTICIPANTS: This prospective cohort study enrolled 690 participants from 175 Maryland households with 1 or more children aged 0 to 4 years between November 24, 2020, and October 15, 2021. For 8 months after enrollment, participants completed weekly symptom questionnaires and submitted self-collected nasal swabs for SARS-CoV-2 qualitative real-time reverse transcriptase polymerase chain reaction (RT-PCR) testing, quantitative RT-PCR testing, and viral lineage determination. For the analyses, SARS-CoV-2 Alpha and Delta lineages were considered variants of interest or concern. Sera collected at enrollment and at approximately 4 months and 8 months after enrollment were assayed for SARS-CoV-2 spike and nucleocapsid protein antibodies.
Incidence, clinical and virological characteristics, and symptoms of SARS-CoV-2 infection by age group and correlations between (1) highest detected viral load and symptom frequency and (2) highest detected viral load and SARS-CoV-2 lineage.
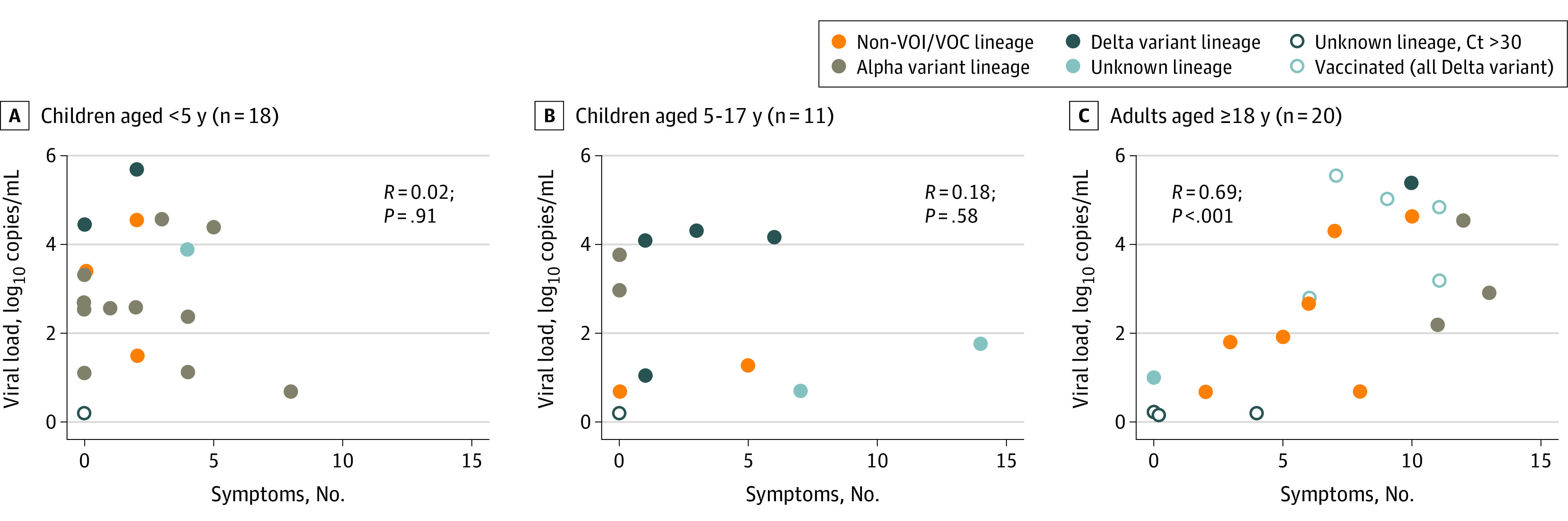
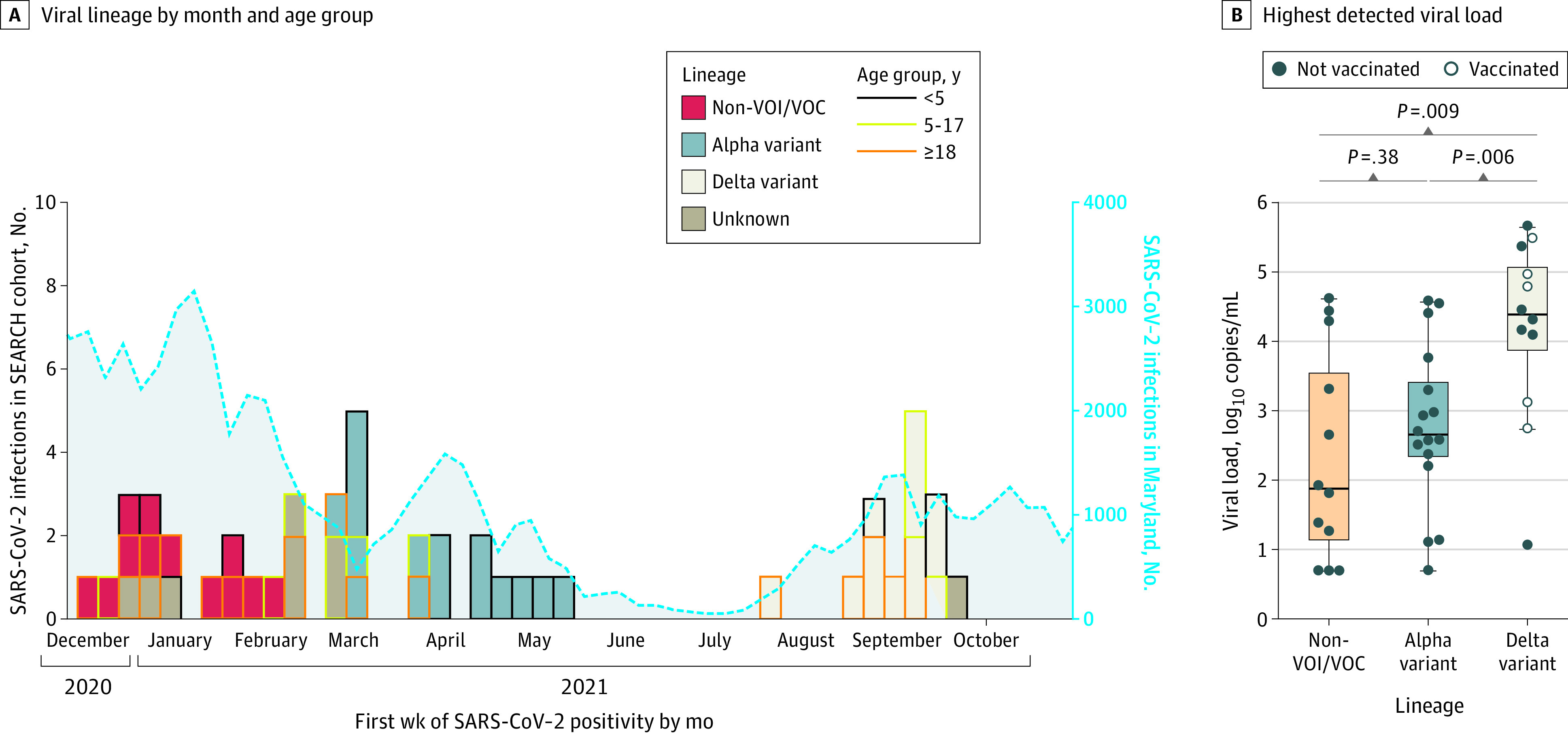
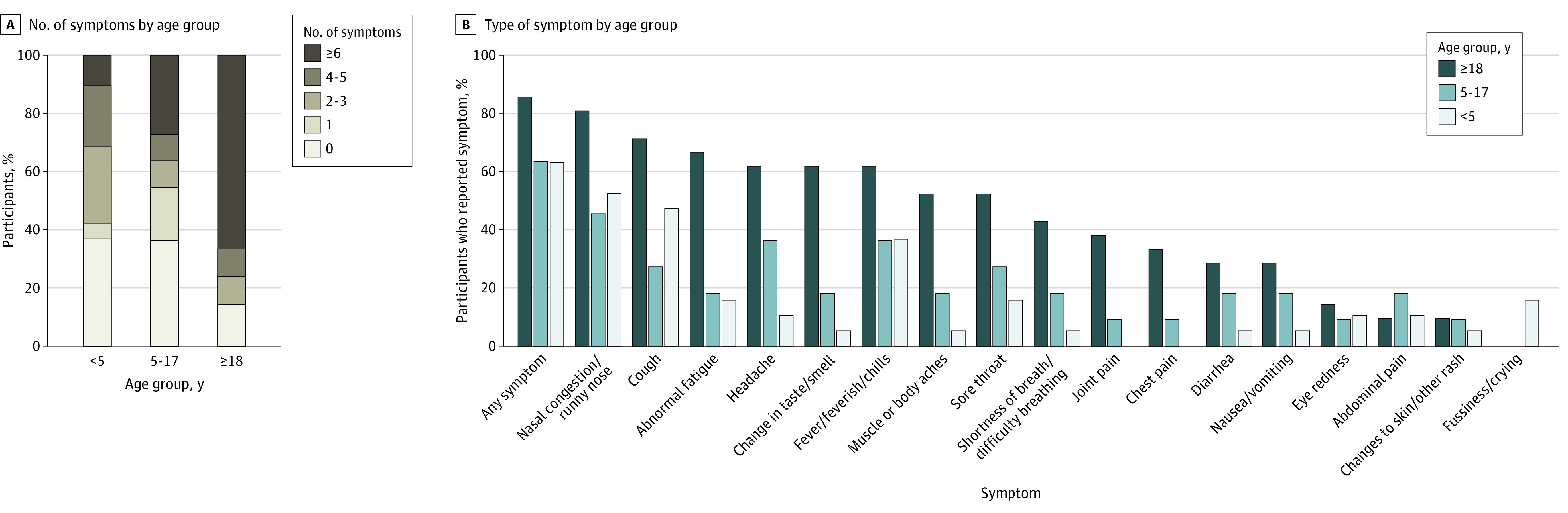
Among 690 participants (355 [51.4%] female and 335 [48.6%] male), 256 individuals (37.1%) were children aged 0 to 4 years, 100 (14.5%) were children aged 5 to 17 years, and 334 (48.4%) were adults aged 18 to 74 years. A total of 15 participants (2.2%) were Asian, 24 (3.5%) were Black, 603 (87.4%) were White, 43 (6.2%) were multiracial, and 5 (0.7%) were of other races; 33 participants (4.8%) were Hispanic, and 657 (95.2%) were non-Hispanic. Overall, 54 participants (7.8%) had SARS-CoV-2 infection during the surveillance period, including 22 of 256 children (8.6%) aged 0 to 4 years, 11 of 100 children (11.0%) aged 5 to 17 years, and 21 of 334 adults (6.3%). Incidence rates per 1000 person-weeks were 2.25 (95% CI, 1.28-3.65) infections among children aged 0 to 4 years, 3.48 (95% CI, 1.59-6.61) infections among children aged 5 to 17 years, and 1.08 (95% CI, 0.52-1.98) infections among adults. Children aged 0 to 17 years with SARS-CoV-2 infection were more frequently asymptomatic (11 of 30 individuals [36.7%]) compared with adults (3 of 21 individuals [14.3%]), with children aged 0 to 4 years most frequently asymptomatic (7 of 19 individuals [36.8%]). The highest detected viral load did not differ between asymptomatic vs symptomatic individuals overall (median [IQR], 2.8 [1.5-3.3] log10 copies/mL vs 2.8 [1.8-4.4] log10 copies/mL) or by age group (median [IQR] for ages 0-4 years, 2.7 [2.4-4.4] log10 copies/mL; ages 5-17 years: 2.4 [1.1-4.0] log10 copies/mL; ages 18-74 years: 2.9 [1.9-4.6] log10 copies/mL). The number of symptoms was significantly correlated with viral load among adults (R = 0.69; P < .001) but not children (ages 0-4 years: R = 0.02; P = .91; ages 5-17 years: R = 0.18; P = .58). The highest detected viral load was greater among those with Delta variant infections (median [IQR], 4.4 [3.9-5.1] log10 copies/mL) than those with infections from variants not of interest or concern (median [IQR], 1.9 [1.1-3.6] log10 copies/mL; P = .009) or those with Alpha variant infections (median [IQR], 2.6 [2.3-3.4] log10 copies/mL; P = .006).
In this study, SARS-CoV-2 infections were frequently asymptomatic among children aged 0 to 4 years; the presence and number of symptoms did not correlate with viral load. These findings suggest that symptom screening may be insufficient to prevent outbreaks involving young children.
很少有研究前瞻性评估 0 至 4 岁儿童的社区 SARS-CoV-2 感染情况。关于年幼儿童 SARS-CoV-2 发病率、临床和病毒学特征以及症状的信息,有助于指导预防和缓解策略。
评估前瞻性家庭队列中 SARS-CoV-2 的发病率、临床和病毒学特征和症状,并比较年幼儿童、年龄较大儿童和成年人的病毒载量、症状和 SARS-CoV-2 谱系。
设计、地点和参与者:本前瞻性队列研究纳入了 2020 年 11 月 24 日至 2021 年 10 月 15 日期间来自马里兰州 175 个家庭的 690 名 0 至 4 岁的 1 名或多名儿童。在入组后 8 个月期间,参与者每周完成症状问卷,并提交自我采集的鼻拭子,用于 SARS-CoV-2 定性实时逆转录酶聚合酶链反应(RT-PCR)检测、定量 RT-PCR 检测和病毒谱系确定。在分析中,SARS-CoV-2 Alpha 和 Delta 谱系被认为是关注或关注的变异。在入组时和入组后约 4 个月和 8 个月收集的血清中检测 SARS-CoV-2 刺突和核衣壳蛋白抗体。
按年龄组和(1)最高检测病毒载量与症状频率和(2)最高检测病毒载量与 SARS-CoV-2 谱系之间的相关性,评估 SARS-CoV-2 感染的发病率、临床和病毒学特征以及症状。
在 690 名参与者(355 [51.4%] 女性和 335 [48.6%] 男性)中,256 名(37.1%)为 0 至 4 岁儿童,100 名(14.5%)为 5 至 17 岁儿童,334 名(48.4%)为 18 至 74 岁成年人。共有 15 名参与者(2.2%)为亚洲人,24 名(3.5%)为黑人,603 名(87.4%)为白人,43 名(6.2%)为多种族,5 名(0.7%)为其他种族;33 名参与者(4.8%)为西班牙裔,657 名(95.2%)为非西班牙裔。总的来说,54 名参与者(7.8%)在监测期间感染了 SARS-CoV-2,包括 22 名(8.6%)0 至 4 岁儿童、11 名(11.0%)5 至 17 岁儿童和 21 名(6.3%)成年人。0 至 4 岁儿童的发病率为每 1000 人-周 2.25 例(95%CI,1.28-3.65),5 至 17 岁儿童的发病率为每 1000 人-周 3.48 例(95%CI,1.59-6.61),成年人的发病率为每 1000 人-周 1.08 例(95%CI,0.52-1.98)。SARS-CoV-2 感染的 0 至 17 岁儿童更常无症状(30 名中有 11 名[36.7%]),而成年人中无症状者(21 名中有 3 名[14.3%])较少,0 至 4 岁儿童最常无症状(19 名中有 7 名[36.8%])。无症状者与有症状者之间(中位数[IQR],2.8[1.5-3.3]log10 拷贝/mL 比 2.8[1.8-4.4]log10 拷贝/mL)或按年龄组(0-4 岁的中位数[IQR],2.7[2.4-4.4]log10 拷贝/mL;5-17 岁的中位数[IQR],2.4[1.1-4.0]log10 拷贝/mL;18-74 岁的中位数[IQR],2.9[1.9-4.6]log10 拷贝/mL)的最高检测病毒载量无差异。成人中病毒载量与症状数量呈显著相关性(R=0.69;P<0.001),但儿童(0-4 岁:R=0.02;P=0.91;5-17 岁:R=0.18;P=0.58)中无相关性。Delta 变异感染的最高检测病毒载量(中位数[IQR],4.4[3.9-5.1]log10 拷贝/mL)大于非关注或关注变异感染(中位数[IQR],1.9[1.1-3.6]log10 拷贝/mL;P=0.009)或 Alpha 变异感染(中位数[IQR],2.6[2.3-3.4]log10 拷贝/mL;P=0.006)。
在这项研究中,0 至 4 岁儿童的 SARS-CoV-2 感染常无症状;症状的存在和数量与病毒载量无关。这些发现表明,症状筛查可能不足以预防涉及幼儿的暴发。