Houston Methodist Pulmonary Transplant Center, Houston Methodist Hospital, Houston, TX.
Department of Academic Pulmonology, Houston Methodist Hospital, Houston, TX.
Crit Care Med. 2022 Nov 1;50(11):1545-1554. doi: 10.1097/CCM.0000000000005660. Epub 2022 Aug 29.
Respiratory failure is a lethal complication of COVID-19 that has remained resistant to drug therapy. Vasoactive intestinal peptide (VIP) is shown in nonclinical studies to upregulate surfactant production, inhibit cytokine synthesis, prevent cytopathy, and block replication of the severe acute respiratory syndrome coronavirus 2 virus in pulmonary cells. The study aims to determine whether Aviptadil (synthetic VIP) can improve survival and recovery in patients with COVID-19 respiratory failure compared with placebo and demonstrate biological effects in such patients.
A multicenter, placebo-controlled trial.
Ten U.S. hospitals: six tertiary-care hospitals and four community hospitals.
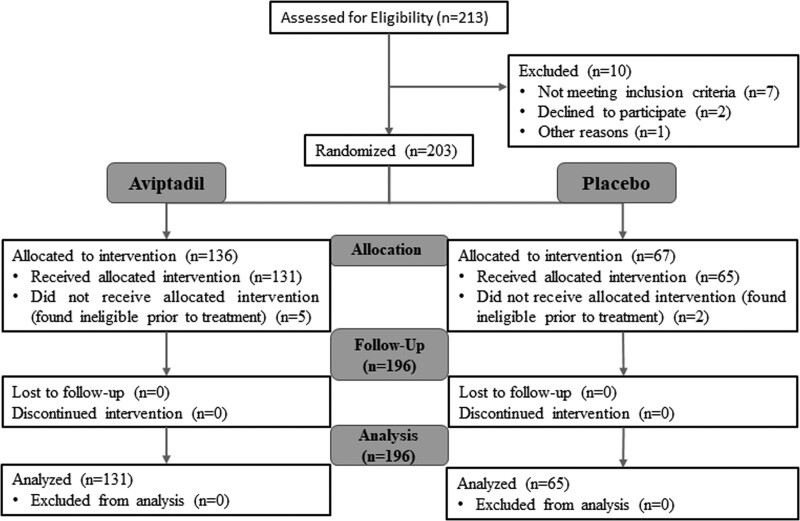
A total of 196 patients with COVID-19 respiratory failure.
Participants were randomized 2:1 to receive 3 days of IV Aviptadil or placebo.
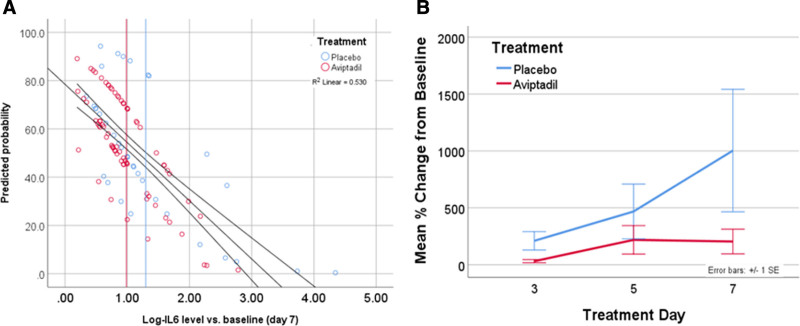
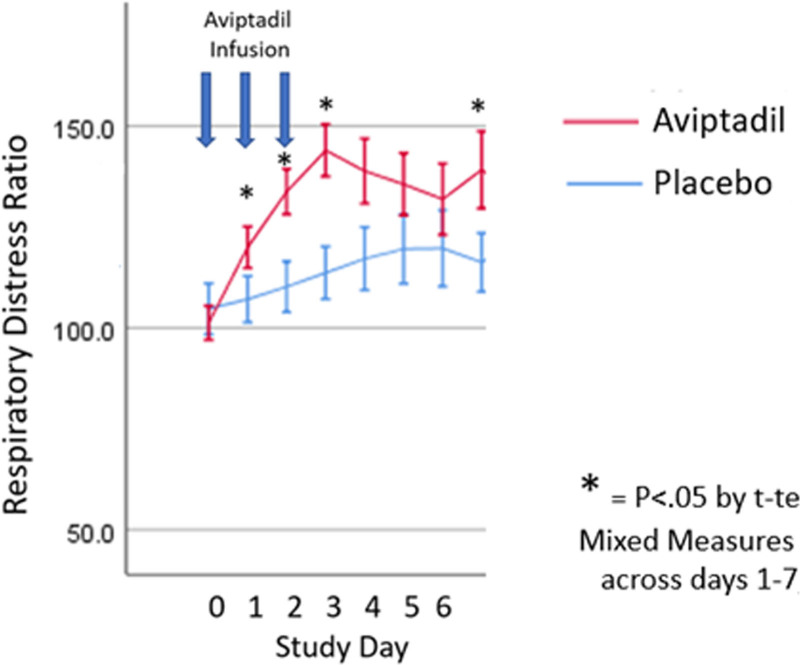
The primary end point (alive and free from respiratory failure at day 60) did not reach statistical significance (odds ratio [OR], 1.6; 95% CI, 0.86-3.11) for patients treated with Aviptadil when controlling for baseline ventilation status as prespecified in the protocol. There was, however, a statistically significant two-fold odds of improved survival (OR, 2.0; 95% CI, 1.1-3.9) at 60 days ( p = 0.035). There was significant improvement in respiratory distress ratio and reduced interleukin 6 cytokine release ( p = 0.02) by day 3.Subgroup analysis identified a statistically significant likelihood of achieving primary end point among those treated with high-flow nasal oxygen at baseline ( p = 0.039). Subjects on mechanical ventilation also experienced a 10-fold increased odds of survival with drug versus placebo ( p = 0.031).
The primary end point did not reach statistical significance, indicating that there was no difference between Aviptadil versus placebo. However, Aviptadil improves the likelihood of survival from respiratory failure at day 60 in critical COVID-19 across all sites of care. Given the absence of drug-related serious adverse events and acceptable safety profile, we believe the benefit versus risk for the use of Aviptadil is favorable for patient treatment.
呼吸衰竭是 COVID-19 的一种致命并发症,一直对药物治疗有抵抗力。在非临床研究中,血管活性肠肽 (VIP) 被证明可上调表面活性剂的产生、抑制细胞因子的合成、预防细胞病变,并阻断严重急性呼吸综合征冠状病毒 2 病毒在肺细胞中的复制。本研究旨在确定与安慰剂相比, Aviptadil(合成 VIP)是否可以改善 COVID-19 呼吸衰竭患者的存活率和恢复率,并证明其对这些患者具有生物学作用。
多中心、安慰剂对照试验。
美国的 10 家医院:6 家三级保健医院和 4 家社区医院。
共有 196 名 COVID-19 呼吸衰竭患者。
参与者按 2:1 的比例随机接受 3 天静脉注射 Aviptadil 或安慰剂。
根据方案中预先规定的基线通气状态,主要终点(第 60 天存活且无呼吸衰竭)未达到统计学意义(优势比[OR],1.6;95%CI,0.86-3.11) Aviptadil 治疗的患者。然而,60 天时的存活率有统计学意义的两倍提高(OR,2.0;95%CI,1.1-3.9)(p=0.035)。第 3 天呼吸窘迫比和白细胞介素 6 细胞因子释放显著改善(p=0.02)。亚组分析确定了基线接受高流量鼻氧治疗的患者达到主要终点的可能性具有统计学意义(p=0.039)。接受机械通气的患者也经历了药物与安慰剂相比存活的几率增加了 10 倍(p=0.031)。
主要终点未达到统计学意义,表明 Aviptadil 与安慰剂之间无差异。然而,Aviptadil 提高了所有治疗场所 COVID-19 严重呼吸衰竭患者在第 60 天的存活率。鉴于没有与药物相关的严重不良事件和可接受的安全性,我们认为 Aviptadil 的获益与风险对患者治疗是有利的。