Pergola Pablo E
Renal Associates, PA, San Antonio, TX 78212, USA.
Int J Nephrol. 2022 Aug 22;2022:9457440. doi: 10.1155/2022/9457440. eCollection 2022.
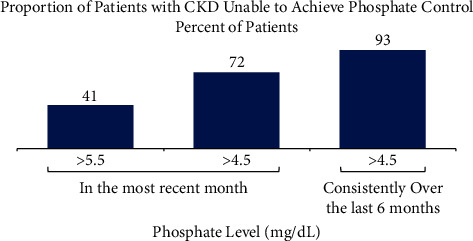
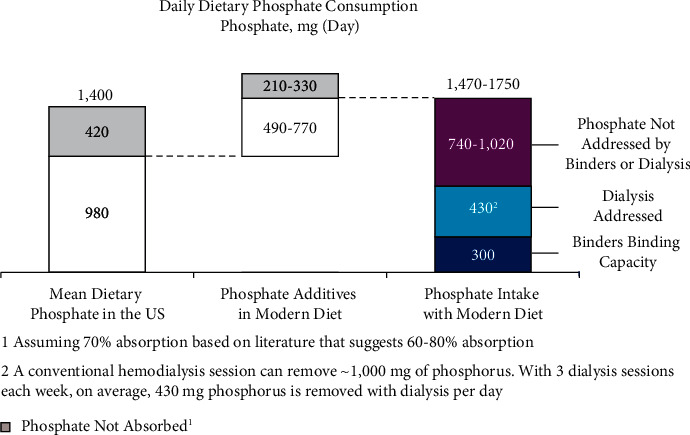
Hyperphosphatemia eventually develops in almost all patients with advanced chronic kidney disease and is associated with negative clinical outcomes. Thus, guidelines recommend targeting treatment to normal phosphate levels in patients with chronic kidney disease. Despite low phosphorus diets, clearance by dialysis, and phosphate binder use, many patients with chronic kidney disease on dialysis are unable to consistently achieve and maintain serum phosphate concentrations <5.5 mg/dL. A chart audit of patients on dialysis receiving phosphate binders showed that 74 to 86% were unable to consistently achieve serum phosphate ≤5.5 mg/dL over 6 months. Furthermore, although there is evidence that serum phosphate concentrations <4.5 mg/dL are associated with improved survival and cardiovascular outcomes, real-world phosphate control data suggest achieving and maintaining this goal for most patients would be extremely challenging, if not near impossible, using current therapies. As phosphate binders can only remove approximately 300 mg of the 2,500 mg or more daily dietary phosphate intake, therapeutic innovations are necessary to improve phosphate management. We present treatment options to complement current therapies including tenapanor, a novel sodium/hydrogen exchanger isoform 3 inhibitor that blocks the dominant paracellular phosphate absorption pathway and has been shown to reduce phosphate levels in several clinical trials.
几乎所有晚期慢性肾脏病患者最终都会出现高磷血症,并伴有不良临床结局。因此,指南建议针对慢性肾脏病患者将治疗目标设定为使血磷水平正常。尽管采用了低磷饮食、透析清除以及使用磷结合剂,但许多接受透析的慢性肾脏病患者仍无法持续实现并维持血清磷浓度<5.5mg/dL。一项对接受磷结合剂治疗的透析患者的图表审查显示,74%至86%的患者在6个月内无法持续实现血清磷≤5.5mg/dL。此外,尽管有证据表明血清磷浓度<4.5mg/dL与生存率提高和心血管结局改善相关,但实际的磷控制数据表明,使用当前疗法,要让大多数患者实现并维持这一目标极具挑战性,甚至几乎不可能。由于磷结合剂每天只能清除约300mg的2500mg或更多的每日饮食磷摄入量,因此需要治疗创新来改善磷管理。我们介绍了一些补充当前疗法的治疗选择,包括替纳帕诺,这是一种新型的钠/氢交换体3抑制剂,可阻断主要的细胞旁磷吸收途径,并且在多项临床试验中已显示出可降低磷水平。