The Bone Infection Unit, Nuffield Orthopaedic Centre, Oxford University Hospitals, Oxford, UK.
Bone Joint J. 2022 Sep;104-B(9):1095-1100. doi: 10.1302/0301-620X.104B9.BJJ-2022-0396.R1.
Excision of chronic osteomyelitic bone creates a dead space which must be managed to avoid early recurrence of infection. Systemic antibiotics cannot penetrate this space in high concentrations, so local treatment has become an attractive adjunct to surgery. The aim of this study was to present the mid- to long-term results of local treatment with gentamicin in a bioabsorbable ceramic carrier.
A prospective series of 100 patients with Cierny-Mader Types III and IV chronic ostemyelitis, affecting 105 bones, were treated with a single-stage procedure including debridement, deep tissue sampling, local and systemic antibiotics, stabilization, and immediate skin closure. Chronic osteomyelitis was confirmed using strict diagnostic criteria. The mean follow-up was 6.05 years (4.2 to 8.4).
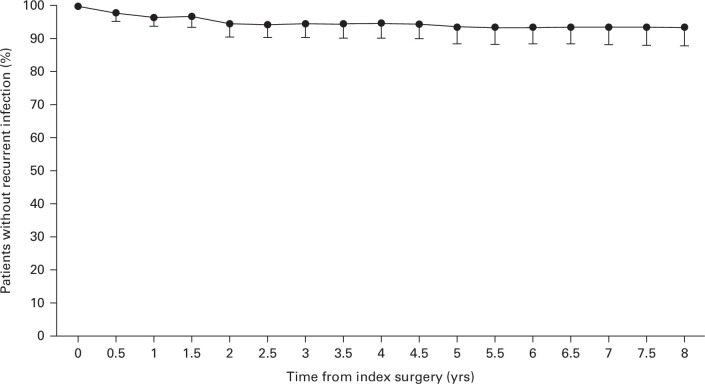
At final follow-up, six patients (six bones) had recurrent infection; thus 94% were infection-free. Three infections recurred in the first year, two in the second year, and one 4.5 years postoperatively. Recurrence was not significantly related to the physiological class of the patient (1/20 Class A (5%) vs 5/80 Class B (6.25%); p = 0.833), nor was it significantly related to the aetiology of the infection, the organisms which were cultured or the presence of nonunion before surgery (1/10 with nonunion (10%) vs 5/90 without nonunion (5.6%); p = 0.570). Organisms with intermediate or high-grade resistance to gentamicin were significantly more likely in polymicrobial infections (9/21; 42.8%) compared with monobacterial osteomyelitis (7/79 (8.9%); p < 0.001). However, recurrence was not significantly more frequent when a resistant organism was present (1/16 for resistant cases (6.25%) vs 5/84 in those with a microbiologically sensitive infection (5.95%); p = 0.958).
We found that a single-stage protocol, including the use of a high-delivery local antibiotic ceramic carrier, was effective over a period of several years. The method can be used in a wide range of patients, including those with significant comorbidities and an infected nonunion.Cite this article: 2022;104-B(9):1095-1100.
切除慢性骨髓炎的骨组织会形成一个死腔,必须加以处理,以避免早期感染复发。全身抗生素无法在该部位达到高浓度,因此局部治疗已成为手术的有效辅助手段。本研究旨在介绍使用庆大霉素生物可吸收陶瓷载体进行局部治疗的中期至长期结果。
前瞻性系列研究纳入了 100 例 Cierny-Mader Ⅲ型和Ⅳ型慢性骨髓炎患者(105 处骨骼),采用一期清创术治疗,包括深组织取样、局部和全身使用抗生素、固定以及即刻皮肤闭合。采用严格的诊断标准确诊慢性骨髓炎。平均随访时间为 6.05 年(4.2-8.4 年)。
末次随访时,6 例(6 处骨骼)患者发生感染复发,故 94%的患者无感染。3 例感染在术后 1 年内复发,2 例在术后 2 年内复发,1 例在术后 4.5 年复发。感染复发与患者的生理分级无显著相关性(20 例 A 级患者中有 1 例(5%),80 例 B 级患者中有 5 例(6.25%);p=0.833),也与感染的病因、培养出的病原体或术前是否存在骨不连无关(10 例骨不连中有 1 例(10%),90 例无骨不连中有 5 例(5.6%);p=0.570)。在混合感染中,对庆大霉素具有中高度耐药性的病原体更为常见(21 例中有 9 例[42.8%],79 例单一致病菌感染中有 7 例[8.9%];p<0.001)。然而,当存在耐药病原体时,感染复发的频率并没有显著增加(16 例耐药病例中有 1 例[6.25%],84 例微生物敏感感染中有 5 例[5.95%];p=0.958)。
我们发现,包括使用高载量局部抗生素陶瓷载体在内的一期方案,在数年内是有效的。该方法可应用于广泛的患者,包括合并严重合并症和感染性骨不连的患者。
2022;104-B(9):1095-1100。